

 PDF
PDF ePub
ePub Citation
Citation Print
Print


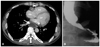
A 47-year-old man with squeezing nature chest pain visited the emergency department. His heart sounds were normal without murmurs, and no history of cardiovascular risk factors or previous heart disease. Initial electrocardiogram showed sinus tachycardia with elevation of ST segment in pre-cordial leads, and he complained of continuous chest pain. Emergent coronary angiography was performed but showed no significant coronary artery stenosis. Transthoracic echocardiography (TTE) showed normal left ventricular dimension and systolic function with relaxation abnormality in mitral inflow Doppler. TTE also showed a round shaped echolucent heterogenous mass lesion, approximately 4.2 × 3.6 cm in size, compressing the left atrium (Fig. 1A). The color Doppler image focusing on the mass lesion revealed an absence of flow. Because of the anatomic location and appearance of the mass lesion, a dilated and extended esophagus and other external cardiac tumor were included in differential diagnosis. TTE was performed after drinking of a liquid containing carbon dioxide to differentiate esophagus from tumor or vascular structure. As result, this mass was identified as the esophagus (Fig. 1B). Chest computed tomography scan revealed diffuse esophageal dilatation compressing the left atrium (Fig. 2A). Gastrografin esophagography showed esophageal dilatation with narrowing of lower esophagus, so called 'bird's beak appearance' (Fig. 2B). High-resolution esophageal manometry demonstrated lack of normotensive lower esophageal sphincter with incomplete relaxation after swallowing consistent with achalasia. Balloon dilatation was performed successfully and patient's symptom was improved. During admission, serial electrocardiograms showed persistent ST elevations with saddle back pattern and Brugada syndrome was suspicious.
Achalasia is a motility disorder characterized by dilatation of distal part of the esophagus with impaired relaxation of the lower esophageal sphincter. Compression of the left atrium leads to various symptoms and signs, which include from mild chest discomfort to hemodynamic instability. There are no previous reports about achalasia compressing left atrium and causes acute chest pain mimicking acute coronary syndrome. TTE is the test of choice for diagnosing the left atrial compression by various etiology.1-3) Furthermore, the esophagus can be identified by the appearance of air contrast during the ingestion of liquid containing carbon dioxide.3) Echocardiography enables clinicians to successfully make the differential diagnosis in patients with chest pain.

 XML Download
XML Download