

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Blood cysts of the heart are commonly reported at postmortem findings in infants. They regress spontaneously in most of the affected patients by the age of 6 months and are rare in adults.1)2) Most often, blood cysts within the heart occur on valves or supporting structures of the valve.3) Blood cysts are often asymptomatic but a few cases resulting in embolization and valvular dysfunctions have been reported.4)5)
We present a patient with a blood cyst attached to the subvalvular apparatus of the anterior mitral leaflet, which was incidentally discovered during a chest computed tomography (CT) performed for the evaluation of fever.
Case
A 47-year-old man presented with fever and cough of three weeks duration and was admitted to a local hospital. Chest CT scan was performed and revealed a 4 cm sized thick-walled cavity in the right upper lobe of the lung with a small amount of fluid accumulation. A 2 cm sized round mass in the left ventricle of the heart was also seen. He was diagnosed with lung abscess and was treated with intravenous antibiotics for 1 week. Consequently, his symptoms completely resolved.
He was referred to our hospital for the incidental cardiac mass. He denied having chest discomfort, palpitation, dyspnea on exertion, or other cardiac symptoms. His medical history was notable only for the lung abscess one month ago. No history of cerebrovascular or cardiac disease, or trauma was noted.
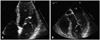
On admission, the blood pressure was 110/70 mmHg, pulse rate was 78 per minute, respiratory rate was 16 breaths per minute, and body temperature was 36.6℃. Cardiac examination revealed no thrills or murmurs. Neurologic examination was completely normal. Laboratory values revealed normal blood chemistry and blood count. Liver function tests and coagulation profiles were within normal limits. C-reactive protein levels was < 0.02 mg/dL (0.01-0.47 mg/dL) and erythrocyte sedimentation rate was 6 mm/h (0-15 mm/h). Chest radiograph showed normal heart size and no cavitary lesion or pneumonic infiltration. Low dose chest CT scan was performed and showed significant regression of the previous cavitary lesion in the right lung. Electrocardiogram showed a normal sinus rhythm. Transthoracic echocardiogram showed a large mobile cystic mass with small calcification attached to the anterior mitral leaflet. The same examination revealed normal mitral valve function with normal ventricular size and function. Transesophageal echocardiogram confirmed the existence of a mobile, round, cystic and pedunculated mass (14 × 16 mm) with hyperechogenic walls and hypoechogenic content attached to the chordal structures of the anterior mitral leaflet and tip of the anterolateral papillary muscle without hemodynamic significance (Fig. 1).
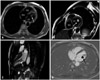
A cardiac magnetic resonance imaging revealed an 18 × 15 mm sized lobulated mass attached to the chordae tendinae, between the anterior leaflet of the mitral valve and anterolateral papillary muscle. The mass showed intermediate signal intensity (SI) on T1 weighted image and high SI on T2 weighted image. The mass showed no definite contrast enhancement after contrast infusion (Fig. 2).
During surgery, the cyst was seen attached to the chordal structures of the anterior mitral leaflet and tip of the anterolateral papillary muscle. The cystic mass was round to oval shaped, measured 1.5 cm in diameter, purple in color and the cyst wall was translucent enough to show its dark blue content. The outer surface was smooth and glistening (Fig. 3A). The cystic mass was successfully resected and a mitral valvuloplasty with neochordae formation and using Carpentier-Edwards Physio annuloplasty ring was performed (Fig. 3B). The cyst cavity was filled with old blood and serosanguineous fluid and showed a small yellowish calcified body in the cyst wall (Fig. 3C).
Microscopically, the unilocular cyst wall was composed of a dense layer of connective tissue with internal flat lining cells. Underneath the lining cells, a blood-filled cystic cavity surrounded by a myxoid stroma was found (Fig. 3D). Immunostaining using standard avidin-biotin-peroxidase complex methods with antibodies against pancytokeratin and cluster of differentiation 31 (CD31) was done. The flat lining cells were stained with CD31 antibody (Fig. 3E). CD31 is highly expressed on endothelial cells and are concentrated at the junctions between them.6) The results were consistent with endothelial cells lining the blood cyst. The patient had an uneventful recovery from the operation and has been maintained on anticoagulation therapy for 1 month and after 1 month, anticoagulation therapy was discontinued. He has been maintained on aspirin 100 mg. The patient has had no symptoms or recurrent intracardiac masses for the 8 month since the excision.
Discussion
Intracardiac blood cysts are usually asymptomatic, small and congenital. They are mainly seen during autopsy in fetuses and infants under the age of 6 months. The cysts regress spontaneously in most patients and are consequently rare in adults.1)2) Elsässer7) first reported a blood-filled cyst of the heart valve in 1844. Since then, similar cyst growth have been reported and potential complications include valve dysfunction, left ventricular outflow tract obstruction, and embolic stroke have been documented.3-5)
Several hypotheses have been proposed to explain the development of blood cysts.4)8)9) The first is that blood cysts are formed during valve development as a result of blood being pressed and trapped in crevices that are later sealed off. This hypothesis could be a plausible explanation for cysts in infants. The second hypothesis is that blood cysts are the result of hematoma formation in the subvalvular region secondary to the occlusion of small vascular branches of end arteries due to inflammation, vagal stimulation, anoxia, or hemorrhagic events. The third hypothesis involves possible heteroplastic changes in the tissue that comes from primitive pericardial mesothelium. The fourth and fifth hypotheses are that these blood cysts simply represent ectatic or dilated blood vessels in the valve or that they represent angiomas. However, there is still no consensus regarding the development of blood cysts.
Paşaoğlu et al.10) suggested surgical removal of a cardiac blood cyst at the time of diagnosis even if the patient is asymptomatic. On the other hand, Dencker et al.4) suggested that a conservative approach in asymptomatic patient with minor cyst, and surgical resection should be considered if symptoms exist or if the cysts lead to any cardiac dysfunction.
We report our incidentally discovered blood cyst. Although our patient was asymptomatic and the cyst did not interfere with the cardiac function, our patient wanted surgical resection of the cardiac mass to rule out primary cardiac malignancy and to prevent possible complications.
Blood cysts are rarely reported, so there is no consensus or guidelines for the optimal management of asymptomatic cases. According to some case reports, depending on which area of the heart is affected, blood cysts may result in a variety of clinical phenomena, including embolism, valvular dysfunction and heart block.11) Therefore surgical resection should be considered in patients with symptoms or valvular dysfunction and resection is also suggested to rule out malignancy.

 XML Download
XML Download