

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Nonalcoholic fatty liver disease (NAFLD) is the most common cause of abnormal liver function tests in adults and almost one third of the population in the Korean has hepatic steatosis.1)2) NAFLD is commonly associated with visceral obesity, dyslipidemia, insulin resistance, and type 2 diabetes and may represent another component of the metabolic syndrome (MetS),3-5) a condition associated with a high cardiovascular risk and, in particular, an increased prevalence of carotid lesions.6) It is important to determine whether NAFLD is an independent predictor of cardiovascular morbidity and mortality and several studies have suggested that there is an association between NAFLD and cardiovascular disease.6-11) Noninvasively detected increased carotid intima media thickness (IMT) is generally accepted as an early indicator of generalized atherosclerosis and has been related to cardiovascular risk factors, and cardiovascular disease including incidence of myocardial infarction and stroke.12-14) Some case-controlled and cross-sectional studies6-8) showed a relationship between NAFLD and carotid IMT.7)11)15) Indeed, it is hypothesized that NAFLD is not merely a marker of cardiovascular disease but may also be involved in its pathogenesis.8) A possible relationship between NAFLD and carotid lesions might have important practical consequences, considering the frequent incidental finding of hepatic steatosis in subjects undergoing abdominal ultrasound (US) for any reason. In these subjects, an US assessment of carotid arteries might also be advisable. However, some degree of variability about the mean carotid IMT values has been observed among all the published reports that result in a difficult evaluation of the magnitude of the observation. For instance, among the different studies, mean carotid IMT values in NAFLD patients range from 0.64 ± 0.10 mm to 1.24 ± 0.13 mm.7)15) It seems to be important to decide whether further recommendations with regard to carotid atherosclerosis screening should be implemented in all NAFLD patients, as currently available epidemiological data indicate that a value of carotid IMT at or above 1 mm at any age is associated with a significantly increased risk of myocardial infarction and/or cerebrovascular disease.14) Thus, we studied a random group of consecutive outpatients undergoing abdominal US to establish the strength of the increased carotid IMT defined ≥ 1 mm and carotid plaque observed in NAFLD patients. In addition, we evaluated whether such an association is independent of classical risk factors and MetS features.
Methods
Study population
From January 2010 to December 2010, we performed a cross-sectional analysis on consecutive 320 non-diabetic NAFLD outpatients (192 men and 128 women, ages 53.5 ± 9.25 years) who received abdominal and carotid US assessment in Maryknoll Medical Center for health screening. The NAFLD diagnosis was based on abdominal US and exclusion of other known etiologic factors of chronic liver disease (alcohol abuse or intake > 40 g/week, viral hepatitis, autoimmune hepatitis, and use of hepato-toxic drugs). No patients had clinical evidence of diabetes mellitus (DM), advanced liver or renal disease, cardiovascular events, or recent history of acute illness. The control group, also recruited from health screening centers consisted of 313 apparently healthy subjects comparable for age and sex with normal liver US/liver function tests and drinking less than 40 g alcohol/week. The study protocol was approved by the ethics review boards of Maryknoll Medical Center, and written informed consent was obtained from all patients enrolled.
Clinical measurements and laboratory procedures
Body mass index (BMI) was calculated by dividing weight in kilograms by the square of height in meters. Waist circumference was measured in a standing position at the level of the umbilicus. Blood pressure (BP) was measured with a standard mercury manometer. Subjects were considered to have hypertension if their BP was ≥ 140/≥ 90 mmHg as recommended by the Joint National Committee VII or if they were on treatment for hypertension. Information on daily alcohol consumption and other lifestyle characteristics were obtained from all participants by questionnaire.4) Venous blood was drawn in the morning after an overnight fast. Plasma liver function tests and glucose, total cholesterol, triglycerides, low density lipoprotein (LDL) and high density lipoprotein (HDL) were determined by standard laboratory procedures. Normal ranges for aspartate aminotransferase, alanine aminotransferase (ALT), and γ-glutamyltransferase (γ-GTP), in our laboratory, were 10-35 units/L for female subjects and 10-50 units/L for male subjects, respectively. The American Diabetes Association criteria were used to define DM and we considered a subject to have DM when the fasting plasma glucose levels were ≥ 126 mg/dL in 2 consecutive assessments or if they were on treatment for DM. The presence of dyslipidemia was assumed if subjects were taking lipid-lowering drugs, or high cholesterol level. Smoking was categorized into the 3 following levels: never smoked, up to 20 pack-years and more than 20 pack-years. Adopting international diabetes federation criteria,16) the metabolic syndrome in South Korean adults was defined by central obesity (waist circumference ≥ 90 cm for men and ≥ 85 cm for women)17) plus two of the following four factors: serum triglyceride ≥ 150 mg/dL, HDL cholesterol < 40 mg/dL for men and < 50 mg/dL for women, systolic BP ≥ 130 mmHg or diastolic BP ≥ 85 mmHg, and fasting plasma glucose ≥ 100 mg/dL.
Ultrasound evaluation
All subjects underwent abdominal and carotid US in order to assess hepatic steatosis and carotid IMT measurement or analysis for the presence of plaques. We used Accuson Sequoia (Siemens, Mountain View, CA, USA), with convex probes (2.5-5 MHz) to scan the liver, and Vivid 7 (GE Medical System, Milwaukee, WI, USA) equipped with a 7 to 12-Mhz linear-array scanner, with a limit of detection of < 0.1 mm to scan carotid arteries. All investigations were performed by two experienced operators (for abdominal and carotid US), blinded to each other regarding the respective US measurements and unaware of patients' clinical data. Following the American gastroenterological association classification of NAFLD,18) NAFLD was defined as the presence of diffuse hyperechoic echo-texture, bright liver,19) increased liver echo-texture compared with the kidneys, vascular blurring and deep attenuation of the ultrasonic beam.
For carotid US, all subjects were examined in a supine position, neck extended, and the chin facing the counter lateral side. Carotid arteries were examined bilaterally in the longitudinal and transversal planes. The common, internal, and external carotid arteries were examined for evidence of atherosclerotic lesions as seen in thickness of the IMT of the common carotid artery, internal carotid artery and external carotid artery and plaque presence. After placing the region of interests in the far wall of the common carotid artery (CCA), mean IMT was estimated in a region free of atherosclerotic plaques with the use of an automatic tracking system.20) Mean IMT was averaged from mean CCA IMT in both far wall, and maximum IMT was defined as the thickest IMT regardless of sites. The increased IMT was considered as ≥ 1.0 mm in either or both carotid arteries and the presence of atherosclerotic plaque was defined as localized lesions with protrusion into the arterial lumen or IMT greater than 1.5 mm.21) Carotid stenosis was not included in the analysis, because no subjects had severe stenosis (≥ 50%).
Statistical analysis
Data were expressed as mean values ± standard deviation and frequencies were expressed as percentages. All analyses were performed using a SPSS 13.0 package program (IBM corp., Armonk, NY, USA). Statistical analysis between the groups was performed using student's t-test for continuous variables and the chi-square test for categorical data. Statistical correlations were determined by the nonparametric Spearman test. Multiple linear regression analysis was performed with respect to carotid IMT and age, BP, BMI, waist circumference, lipid profile, liver enzymes, and the presence of NAFLD were included as covariates. The independence of the associations of variables with abnormal IMT and presence of plaque, considered as the dependent variable, was also assessed by binary logistic regression analyses and age, BP, BMI, waist circumference, lipid profile, liver enzymes, and the presence of NAFLD were included as covariates. Separate regression models were tested in two groups of patients according to the presence of MetS. Probability levels lower than 0.05 were considered significant.
Results
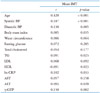
The baseline characteristics of participants are shown in Table 1. Because of the study design, NAFLD and control subjects were comparable in terms of age and sex. Significantly higher BMI, BP, liver enzymes and high sensitivity C-reactive protein (hs-CRP), lipid profiles were found in the subjects with NAFLD. Smoking history, microalbuminuria, and medications did not differ between the groups. NAFLD patients had a significantly increased carotid IMT (mean IMT: 0.79 ± 0.18 vs. 0.73 ± 0.13 mm, maximal IMT: 0.99 ± 0.38 vs. 0.86 ± 0.22 mm; all p < 0.001) and the prevalence of MetS (50.9% vs. 18.2%, p < 0.001) than those without the condition. The prevalence of increased IMT and carotid plaque were 52.5% and 34.1% in the patients with NAFLD vs. 35.8% and 18.8% in the patients without this condition (p < 0.001). As shown in Table 2, the difference in IMT and prevalence of plaque were also significant even without MetS as well as subjects with MetS (all p < 0.05). The lowest level of carotid IMT was found in control subjects without MetS, intermediate in NAFLD patients with without MetS, and highest in those with NAFLD patients with MetS (Table 2).
Association between the NAFLD and carotid atherosclerosis
Age was strongly correlated with mean IMT (r = 0.420, p < 0.001) and maximal IMT (r = 0.402, p < 0.001). Systolic and diastolic BP, BMI, waist circumference, triglycerides, LDL cholesterol and hs-CRP showed modest correlation with mean IMT (Table 3). IMT was also positively correlated with liver enzymes such as ALT and γ-GTP and was inversely associated with HDL cholesterol (all p < 0.05) (Table 3). In multiple linear regression analysis, the presence of NAFLD was significantly associated with carotid IMT after adjustment of age, BP, BMI, waist circumference, lipid profile, liver enzymes and hs-CRP (all p < 0.05) (Table 4).
The utility of NAFLD findings in identifying patients with carotid artery atherosclerosis with or without MetS was assessed further by determining the sensitivity, specificity, positive predictive value, and odds ratio (Table 5). By binary linear logistic regression analysis, NAFLD-associated adjusted odds ratio for increased IMT was 1.236 [95% confidence interval (CI), 1.023-1.467, p = 0.016] without MetS (R2 = 0.299, adjusted R2 = 0.222) and 1.178 (95% CI, 1.059-1.311, p = 0.003) with MetS (R2 = 0.351, adjusted R2 = 0.263) after adjustment of age, BP, BMI, waist circumference, lipid profile, liver enzymes. NAFLD-associated adjusted odds ratio of carotid plaque was 1.583 (95% CI, 1.309-1.857, p = 0.024) without MetS (R2 = 0.281, adjusted R2 = 0.192) and 1.536 (95% CI, 0.512-4.604, p = 0.444) with MetS (R2 = 0.270, adjusted R2 = 0.196). The value of variation inflation factor was less than 10 in age, BP, BMI, waist circumference, lipid profile, and liver enzymes in every cases.
Discussion
Our study demonstrated that an incidental finding of NAFLD is associated with carotid artery atherosclerosis in non-diabetic outpatients undergoing abdominal US assessment for health screening, even without MetS, after adjustment for a broad spectrum of potential confounders. These findings not only support the view of NAFLD as a hepatic manifestation of MetS,9) but also suggest that hepatic fat accumulation is atherogenic beyond its association with insulin resistance.
An association between NAFLD and carotid IMT has already been reported in some previous studies,6-11)15) and even in children.22) Although Targher et al.6) found a significant increase in carotid IMT in the presence of NAFLD in non-obese healthy volunteers, the other study reported that the association between NAFLD and carotid IMT concerned only the patients with MetS.11) The same relationship is absent or present but largely explained by insulin resistance, in type 2 diabetic patients,23)24) and Volzke et al.15) described an independent association of hepatic steatosis with carotid plaques, but not with carotid IMT. In the present study, we found that although both MetS and NAFLD were independently associated with carotid IMT, the presence of NAFLD showed independent affect on carotid IMT and plaque in patients without MetS. Also, there was significant positive correlation between ALT and γ-GTP and carotid IMT. These results are supported by previous prospective studies reporting strong associations between elevated serum liver enzymes as surrogate markers of NAFLD2-5) and the incidence of cardiovascular disease (CVD) in both non diabetic and diabetic individuals.25)26) Our results are also supported by recent cross-sectional observations documenting a significant increase in carotid IMT among patients with ultrasonographically diagnosed NAFLD.6)15)27)
Because our study was only designed to ascertain whether an incidental finding of NAFLD in outpatients may suggest the search for carotid lesions, the role of NAFLD in the formation of initial or advanced carotid lesions is not explained. The biological mechanisms of accelerated atherosclerosis contributed by NAFLD are still poorly understood. NAFLD itself might act as a stimulus for further increased whole-body insulin resistance and dyslipidemia, leading to accelerated atherosclerosis. Recent prospective studies demonstrated that raised liver enzymes independently predict the development of the MetS,28)29) implicating that patients with more severe fatty liver disease are those who showed elevated liver function test results. Our result also showed that GTP was associated with carotid atherosclerosis, although the significance was disappeared after adjustment of other confounding factors. However, NAFLD was associated with increased carotid IMT independently classical risk factors and MetS, it is conceivable that other atherogenic mechanisms could be involved. One hypothesis could be a direct link between fatty liver and dyslipidemia, endothelial dysfunction, or oxidative stress, and thus atherosclerosis.30) A strong association between NAFLD and endothelial dysfunction as measured by brachial artery flow mediated vasodilatation, a reliable marker of early atherosclerosis, was also recently described.31)32)
Although the association between NAFLD and early or advanced carotid lesions is not new, we demonstrated this association for the first time in a random group of non-diabetic outpatients undergoing abdominal US for health screening. Despite several previous studies demonstrated the association between NAFLD and carotid IMT and/or carotid plaque, no general consensus exists on the systematic screening of carotid atherosclerosis in patients with fatty liver disease. Our study suggests that an incidental finding of NAFLD was significantly associated with increased carotid IMT (≥ 1 mm) or plaque, which may represent a new indication for performing an assessment to search for silent arterial lesions. Thus, our findings might have important clinical and public health implications, emphasizing the importance of evaluating the CVD risk in patients diagnosed with NAFLD. Currently, it is not known whether improving NAFLD will ultimately prevent the development of CVD. In fact, the only general recommendation for management of NAFLD patients to date is related to lifestyle changes and an attempt at gradual weight loss along with appropriate control of serum glucose and lipid levels.3)33) However, patients with NAFLD having increased carotid IMT could be candidates not only for aggressive treatment of the liver disease, but also for cholesterol lowering and aggressive treatment of underlying CVD risk factors; this would help to modify and potentially decrease the global CVD risk of these patients.
Study limitations
Because our study was cross-sectional, the causative nature of the associations cannot be established. Prospective studies will be required to sort out the time sequence of events. Moreover, carotid US was the optional test in our health screening center, so the patients who received both abdominal and carotid US assessment would have more traditional risk factor for atherosclerosis, which may explain the high prevalence of carotid atherosclerosis in our study subjects. However, it is important to emphasize that the evidence from this strongly supports the possibility that NAFLD could also be atherogenic among NAFLD patients without diabetes.
Another limitation of this study was that the diagnosis of NAFLD was based on the exclusion of known etiologic factors of liver disease and on US examination but was not confirmed by liver biopsy for ethical reasons. Thus, currently it is uncertain whether there is a significant association between early carotid atherosclerosis and the severity of liver histology among NAFLD patients. Clarification of this aspect may help to explain the underlying mechanisms and may be of clinical importance in planning preventive and therapeutic strategies. However, US examination is by far the commonest way of diagnosing NAFLD in clinical practice19) and the presence of > 33% fat on liver biopsy was optimal for radiological detection of steatosis.34) Although US is highly operator-dependent, and the diagnosis of fatty liver is based mainly on the subjective assessment of liver echogenicity, the reliability of US for the detection of fatty liver showed kappa statistics ranging from 0.54 to 0.92 for intrarater reliability and from 0.44 to 1.00 for interrater reliability.35)
In conclusion, NAFLD is significantly associated with carotid atherosclerosis in non-diabetic outpatients even without MetS. Carotid screening for NAFLD might be beneficial for assessment of future atherosclerotic complications, because NAFLD might be a marker of increased carotid IMT and of the presence of carotid plaque in outpatients undergoing abdominal US.




 XML Download
XML Download