

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The clinical application of echocardiography for prenatal imaging has the major advantage that it is non-invasive, easy accessible and can be used in pregnancy to study the fetus in a truly physiological state. A wide variety of echocardiographic methods have been used for evaluation of fetal anatomy and cardiac function.1)
There are several reports about diastolic cardiac function in the human fetal heart. However, the data was different according to investigators.2-7)
Diastolic performances of right and left ventricles change in a fetus and E/A ratio of atrioventricular valves and ventricular diastolic compliance change before and after birth. The majority of diastolic filling during the initial fetal period occurs towards the end diastolic period and this pattern is observed in adults with disease.8-10) A fetus relies on atrial contraction which is used as an additional pump that increases ventricular filling.11) Diastolic pattern of left and right ventricles changes as age increases but the normal diastolic filling pattern present in adults is not observed until 1 year of postnatal life during which diastolic filling pattern constantly changes.11)
Diastolic function is complex and its interpretation by Doppler investigation is challenging in abnormal conditions such as congenital heart diseases, intrauterine growth retardation,12) fetuses of diabetic mothers.13) Gestational diabetes mellitus has been used as a model of diastolic dysfunction in fetuses owing to myocardial hypertrophy and the consequent reduction of ventricular compliance.13)
Pseudonormalization may mask severe dysfunction with reduced compliance and relaxation. Furthermore, Doppler flow velocity patterns are influenced by loading conditions.14)
This study aims to examine the difference in atrioventricular diastolic performances by evaluating the changes in atrioventricular valve flow from gestational age 37-40 weeks to the first month of postnatal life.
Methods
Study population
Fetal echocardiography was prospectively performed in 24 normal human fetuses of gestational age 37-40 weeks and at 1 hour, 6 hours, 24 hours, 3 days, 1 week and 1 month of postnatal life between Jan 2003 and Dec 2008.
Normal pregnant women without diabetes, hypertension or eclampsia were only included and fetuses with cardiac disease and twins were excluded. This study was carried out with the approval of the ethics committee of Ewha Womans University Hospital Institutional Review Board and written informed consents were obtained from all subjects.
Echocardiography
Fetal echocardiography was performed according to standard recommendations15) using IU22 (Philips Medical Systems, Bothwell, WA, USA) with 5 MHz, 3.5 MHz transducers. Sample volume size used in Doppler echocardiography was 2 mm and 100 Hz filter was used. The Doppler beam intercepted blood flow at an angle less than 20 and Doppler echocardiographic measurements were made while the fetus made no movement. The anatomical structure of a normal fetus was confirmed in 4 chamber, short axis, aortic arch and ductal views. Doppler waveform across mitral and tricuspid valves was measured distal to the valves using a 4 chamber view. Peak early filling velocity (E) during the early diastolic phase and peak atrial filling velocity (A) during the late diastolic phase or atrial contraction were measured to assess diastolic function.16) Time-velocity integral (TVI) and heart rate were measured as well.
Statistical analyses
Statistical analyses were performed using the Statistical Package for Social Sciences version (SPSS Inc., Chicago, IL, USA). The average and standard deviation of all measurements were collected. Statistical analysis was done using t-test and a p-value of less than 0.05 was regarded as significant.
Results
Changes in mitral flow
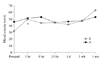
E velocity of prenatal mitral flow was 31.3 ± 8.6 cm/sec and it was 49.5 ± 13.2 cm/sec at 1 hour (p < 0.05), 43.8 ± 12.6 cm/sec at 6 hours, 44.9 ± 11.4 cm/sec at 24 hours, 41.5 ± 12.7 cm/sec at 3 days, 45.8 ± 7.3 cm/sec at 1 week, 62.3 ± 13.1 cm/sec at 1 month of postnatal life (Table 1, Fig. 1).
Changes in tricuspid flow
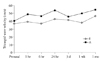
E velocity of prenatal tricuspid flow was 37.1 ± 5.7 cm/sec and it was 39.1 ± 12.4 cm/sec at 1 hour, 36.8 ± 8.6 cm/sec at 6 hours, 42.9 ± 12.4 cm/sec at 24 hours, 41.1 ± 11.9 cm/sec at 3 days, 38.1 ± 9.4 cm/sec at 1 week, 46.2 ± 12.5 cm/sec at 1 month of postnatal life (Table 2, Fig. 3).
A velocity of prenatal tricuspid flow was 40.7 ± 17.7 cm/sec and it was 49.0 ± 14.4 cm/sec at 1 hour, 46.4 ± 6.7 cm/sec at 6 hours, 53.9 ± 9.4 cm/sec at 24 hours, 45.6 ± 16.9 cm/sec at 3 days, 49.9 ± 8.5 cm/sec at 1 week, 54.7 ± 16.3 cm/sec at 1 month of postnatal life (Table 2, Fig. 3).
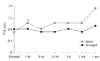
No significant increase in E/A ratio from prenatal to postnatal tricuspid flow was observed as it was 0.8 ± 0.3 at prenatal life, 0.8 ± 0.1 at 1 hour, 0.7 ± 1.3 at 6 hours, 0.7 ± 0.2 at 24 hours, 0.8 ± 0.2 at 3 days, 0.7 ± 0.2 at 1 week and 0.9 ± 1.0 at 1 month of postnatal life. E/A value of tricuspid valve was higher than that of mitral valve before birth but E/A value of mitral valve increased and was higher than that of tricuspid valve after birth (Table 2, Fig. 2).
A-wave dominance in mitral valve before birth quickly changed to E-wave dominance in mitral valve after birth, but A-wave dominance of prenatal tricuspid valve was maintained at least until 1 month of postnatal life. It is shown that diastolic performance and compliance of left ventricle are superior to those of right ventricle after birth.
Time velocity integral
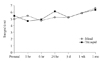
TVI of prenatal mitral flow was 4.9 ± 0.9 cm and it was 5.4 ± 1.4 cm at 1 hour, 4.7 ± 0.8 cm at 6 hours, 5.2 ± 0.8 cm at 3 days, 5.8 ± 1.4 cm at 1 week, 6.5 ± 1.1 cm at 1 month of postnatal life (Table 1, Fig. 4).
TVI of prenatal tricuspid flow was 5.4 ± 2.5 cm and it was 4.6 ± 1.2 cm at 1 hour, 4.8 ± 0.8 cm at 6 hours, 6.1 ± 1.2 cm at 24 hours, 5.2 ± 1.7 cm at 3 days, 5.8 ± 1.1 cm at 1 week, 6.3 ± 1.0 cm at 1 month of postnatal life. TVI of tricuspid flow was significantly higher than that of mitral flow before birth, but there was no difference after birth (Table 2, Fig. 4).
Discussion
In this study, we demonstrated that the dominance of mitral A wave before birth was changed very quickly after birth to the dominance of E wave, but the dominance of tricuspid A wave was maintained at 1 month. Diastolic function and compliance of mitral valve were better than those of the tricuspid valve after birth.
The clinical application of echocardiography has advantage for prenatal diagnosis. It is noninvasive, easy accessible and can be used in pregnancy to study the fetus in a truly physiological state.
Blood flow patterns across atrioventricular valves in normal human fetus is examined as E and late peak A. E is related to preload and active dilation of the ventricular muscle. Late peak A is influenced by atrial contraction and ventricular compliance.17)
Diastolic filling of normal adults without any cardiac disease is divided into 3 phases. Early filling as the first phase consists of responses to pressure difference across atrium and ventricle and early dilation filling as valves open due to suction power following ventricular dilation during which ventricular pressure drops below atrial pressure. Early filling is influenced by the extent of ventricular dilation, ventricular compliance, atrial pressure, cardiac anatomy and pressures and volumes of cardiac structures. Three-fourths of filling occurs at this phase at adulthood. The second phase is referred to as diastasis during which blood flow comes to a halt after early filling phase. The last phase consists of atrial contraction and the remaining one third blood flow is forced into ventricles.18)
The blood flow velocity of late dilation period which coincides with atrial contraction is higher than that of early dilation period across atrioventricular valves. This reflects the decrease in compliance in fetal cardiac dilation.19) The majority of diastolic filling during the initial fetal period occurs towards the end diastolic period and this pattern is observed in adults with disease.8-10) A fetus relies on atrial contraction which is used as an additional pump that increases ventricular filling.18) Diastolic pattern of left and right ventricles changes as age increases but the normal diastolic filling pattern present in adults is not observed until 1 year of postnatal life during which diastolic filling pattern constantly changes.18)
As gestational age increased, E/A value of both mitral and tricuspid valves increased significantly.18) When the late gestation and the immediately period after birth were compared, E/A value of mitral valve significantly increased while that of tricuspid valve did not show a significant change. E/A value of mitral valve increased significantly during the first year after birth and that of tricuspid valve also increased but the increase was insignificant. Comparing mitral and tricuspid valves of fetal and neonatal periods, E/A values showed a significant changes and a greater variation was observed in a fetal period. E/A values of mitral and tricuspid valves exhibited significant differences during the fetal period while no such pattern was observed during the neonatal period.
The data was different according to investigators. Ishii et al.20) reported that although A-wave dominance of prenatal mitral valve quickly changes after birth to E-wave dominance, A-wave dominance of prenatal tricuspid valve is maintained for at least 5 days after birth. Hong10) measured peak early systolic velocity and peak late systolic velocity of mitral valve at 1 day, 1 week and 1 month after birth and reported that the velocities increased significantly over time. E/A values also increased significantly. After one month of postnatal life, left ventricular diastolic function increased analogously to that in childhood. In our study, prenatal mitral A wave dominance changed quickly to E wave dominance after birth as well. However, tricuspid A wave dominance was maintained until at least 1 month after birth. Diastolic function and compliance of left ventricle were superior to those of right ventricle after birth.
According to Veille et al.21) the TVI of mitral and tricuspid flow increases constantly over the fetal period during which the TVI of tricuspid flow is significantly higher than that of mitral flow. Mitral flow TVI increases significantly while that of tricuspid flow shows a constant increase that is statistically insignificant. The TVI of the right ventricle takes dominance in fetal period which changes to the left ventricle TVI dominance in neonatal period. Fernández Pineda et al.9) demonstrated that E and E/A values show a significant linear increase in both mitral and tricuspid valves while A value has no variation during the gestational period. Doppler velocity through tricuspid valve is higher than that through mitral valve. Mitral E/A ratio is greater than that of tricuspid which decreases over time. A value, however, does not change over time and this indicates that tricuspid compliance is maintained. E value influences the E/A value variation and this implies that ventricular dilation, compliance and preload increase over time.
Reed et al.22) reported A wave dominance in 97% of the fetuses studied. Both mitral and tricuspid E/A ratios increase significantly over gestational period. Also, peak E of mitral valve increases according to gestational age while constant.
Diastolic function of a fetus is in accord with compliance which increases over the gestational period.1) E wave, A wave and E/A ratio of tricuspid valve was reported to be significantly higher than those of mitral valve in other studies,23-26) but no significant difference between tricuspid and mitral valves was observed in our study.
The limitation of this study includes the small population size. Inter-observer correlation was not determined in this study because all data were analyzed by the same investigator.
In conclusion, the dominance of mitral A wave before birth was changed very quickly after birth to the dominance of E wave, but the dominance of tricuspid A wave was maintained at 1 month. Diastolic function and compliance of mitral valve were better than those of the tricuspid valve after birth.
Further studies are needed to identify definite predictors of poor prognosis in high-risk pregnancies. Future prospective studies including those with multicenters and a larger population group are warranted.


 XML Download
XML Download