

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
True aneurysms, or diverticulae, of the mitral valve are a rare cause of mitral regurgitation. It occurs most commonly in association with aortic valve infective endocarditis,1-5) but they may also present with mitral valve infective endocarditis,5-7) chronic mitral regurgitation8) or as a complication of mitral valve prolapse.9) The echocardiographic features of mitral valve aneurysms (MVA) are non-specific,3-9) and can be misinterpreted as a large vegetation, cystic left atrial myxoma, or degeneration in association with a prolapsing leaflet. Delay in making the correct diagnosis increases the risk of infection, embolization, or rupture of the aneurysm; these complications can be prevented by surgery to repair or replace the valve.3) We report a patient in whom a MVA of posterior leaflet as initially misdiagnosed as cystic mass, which was confirmed at operation.
Case
A 70-year-old woman presented to the hospital with dyspnea about 3 weeks. She had history of type 2 diabetes mellitus and old cerebral infarction. There was no family history of aortic, collagen, vascular or congenital heart disease. Vital signs were blood pressure of 125/59 mmHg, pulse rate of 98 beat/min, respiration rate of 24 breaths/min, and body temperature of 36.5℃. On the physical examination, there were no peripheral skin lesions and cardiac auscultation revealed a grade 2/6 systolic heart murmur and electrocardiography demonstrated non-specific depression of ST segment and T wave changes. The blood chemistries, including coagulation studies, erythrocyte sedimentation rate, C-reactive protein, the complete blood count, and lipid profiles were within normal limits. A chest radiograph showed increased interstitial markings on both lower lung fields.
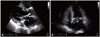
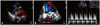
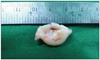
Transthoracic echocardiography showed left ventricular hypertrophy and enlarged left atrium size (44.3 mm) with normal left ventricular ejection fraction (68%). Moderate aortic regurgitation with senile sclerotic aortic valve change, and moderate tricuspid regurgitation with elevated right ventricle systolic pressure (49 mmHg) was shown. Interestingly, a large fluttering cystic mass (1.3 × 1.6 cm) in the left atrium attached to the posterior mitral valve leaflet which bulged into the left atrium and ventricle throughout the cardiac cycle resulted in poor coaptation and opening of mitral valve (Fig. 1). The color Doppler flow showed that the cystic mass was filled with flow during systole and also the color flow in the cystic mass was communicated with the left atrium (Fig. 2). Continuous wave Doppler revealed that the mass caused hemodynamic disturbance and there was moderate increase of mean pressure gradient (Fig. 2C). Because there was no clinical evidence of infective endocarditis with negative blood culture and no history of previous infective endocarditis or rheumatic fever, the cystic mass was considered as cystic left atrial myxoma, less likely MVA. She denied any further cardiac imaging studies including transesophageal echocardiography. Subsequently, she was transferred to the department of thoracic surgery. She was taken to the operating room for left atrial cystic mass resection. At operation, a mobile left atrial mass was identified as MVA (Fig. 3). A small perforation was seen at the aneurysm of posterior mitral leaflet. The aneurysm was resected and mitral valve annuloplasty was done. Histopathologic examination of the resected segments showed myxomatous degenerative change and calcification of mitral valve without evidence of an acute inflammatory process. She made an uneventful postoperative recovery and 2 months later was well with no evidence of mitral regurgitation.
Discussion
MVA, which is defined as a localized bulge of the mitral leaflet toward the left atrium with systolic expansion and diastolic collapse,9) is uncommon and reported cases are rare and often the consequence of infective endocarditis.1-7) Early and preoperative recognition of its presence is important because it may rupture and produce catastrophic mitral regurgitation in an already seriously ill patient or it may be overlooked at the time of aortic valve replacement. Primary or secondary endocarditis from aortic infection, rheumatic disease, and other disorders causing connective tissue degeneration5) are the possible cause from which the strength of the mitral leaflet is weakened and the leaflet protrudes into the left atrium under the left ventricular pressure. There are also occasional reports of the MVA forming in patients without endocarditis, such as those with connective tissue diseases, including mitral valve prolapse, osteogenesis imperfecta, Marfan syndrome, and pseudoxanthoma elasticum.5)10)11) In the absence of endocarditis, a regurgitation aortic jet has been speculated to be the most possible cause of MVA,12) but on the posterior mitral leaflet, any mechanical stress due to aortic regurgitation could be profoundly less compared to that acting on the anterior one. Our case seems to be a very rare incident since the aneurysm was detected on the posterior mitral valve leaflet although the aortic regurgitation was not severe whereas endocarditis was never documented.
Diagnosis of MVA by echocardiography has been reported before.3)4) Echocardiography shows MVA as a localized saccular bulge of the leaflet toward the left atrium and communication between the aneurysm and the left ventricle during the cardiac cycle.3)4) Mitral valve repair or replacement is indicated when aneurysm is ruptured or when the unruptured aneurysm is large or accompanied by significant regurgitation. MVA may be confused with cystic degeneration of the valve, a cystic atrial myxoma, or a large vegetation.13) Our patient shows that transthoracic echocardiography may not be diagnostic in this condition and can be misleading especially when the posterior leaflet is affected.6)8)9)
Until now, we cannot find any report of MVA of posterior leaflet without evidence of infective endocarditis. Our case suggests that MVA could happen on posterior leaflet of the mitral valve without apparent involvement of the aortic valve endocarditis. In conclusion, MVA should be considered in the differential diagnosis of mass lesions seen on the atrial side of the mitral valve at echocardiography.
 XML Download
XML Download