

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cardiac myxoma make a few symptoms. But rarely severe complications like systemic embolism, heart failure, pulmonary hypertension were shown. The signs and symptoms produced by tumors are related to the size and location of the tumors. When situated in the left side of the heart, they may cause symptoms of left atrial outflow obstruction such as pulmonary hypertension. We report one case of severe complications of myxoma in adolescents with severe pulmonary hypertension that were recovered by surgical removal.
Case
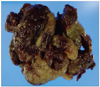
A 14-year-old boy was admitted to our hospital due to sudden onset dyspnea. The patient had no past medical history and family history of lung disease and cardiac disease. Two weeks before admission, he suffered from non-productive cough. At the time, physical findings included a regular heart rate of 98 beats/minutes, a blood pressure of 120/80 mm Hg, respiratory rate of 28/minutes represented tachypnea, a body temperature of 36.4℃, resting oxygen saturation of 96%. He had a palpable four finger sized hepatomegaly, pre-tibial pitting edema. Thoracic auscultation revealed mid-diastolic murmur (Grade II) and inspiratory crackle was audible in both lower lung fields. An electrocardiogram revealed a normal sinus rhythm with right axis deviation, right atrial enlargement. A chest X-ray showed mild cardiomegaly and mild pulmonary congestion (Fig. 1). On laboratory findings, Aspartate Aminotransferase/Alanine Aminotransferase 136/106 IU/L, total bilirubin 1.0 mg/dL, pro-brain nitrouretic peptide 6,291 pg/mL. Transthoracic echocardiography to find cause of murmur showed a nodular, mobile, hyperechoic, 4.34 × 8.11 cm sized left atrial mass (Fig. 2) with moderate tricuspid regurgitation suggestive of pulmonary hypertension (maximal pressure gradient = 81.61 mm Hg, pulmonary artery systolic pressure = 101 mm Hg) (Fig. 4), and markedly enlarged right atrium and right ventricle. Left ventricular ejection fraction and regional wall motion were normal. We performed excisional biopsy for mass evaluation. The mass were grossly composed of several friable hemorrhagic nodular mass, measuring 6 × 5 × 4.5 cm in size (Fig. 6). On microscopic view, the mass were composed of setellate myxoma cells, inflammatory cells, much basophilic substance and slit like vessels that were compatible with myxoma.
After 3 days of mass removal, the follow-up echocardiography showed no visible mass lesion (Fig. 3) with mild tricuspid regurgitation suggestive of decreased pulmonary arterial pressure (pressure gradient = 39.37 mm Hg, pulmonary artery systolic pressure = 54 mm Hg) (Fig. 5).
The postoperative course was uneventful and the patient remained well during the 3 years follow-up period.
Discussion
Myxomas most commonly occur between the third and the sixth decade of life.
Sixty-five percent of cardiac myxomas occur in women and are rare in children.1) Early diagnosis is difficult because the symptoms of atrial myxoma are frequently nonspecific.1)2) Large myxomas may remain asymptomatic if tumour growth is very slow. The heart auscultation can be quite similar to that of mitral valve disease, and may be associated with a tumoral sound. The most useful examination in the diagnosis is the echocardiogram that is highly sensitive and can diagnose up to 100% of the cases. Although histopathologically benign, cardiac myxomas can cause chronic systemic inflamation, embolism or intracardiac obstructions, leading to increased morbidity.3)
The symptoms of left-sided heart failure were usual in patients with left atrial myxomas, such as dyspnea on exertion, may progress to orthopnea, paroxysmal nocturnal dyspnea or pulmonary edema because of obstruction at the mitral valve orifice.4)5)
Dyspnea on exertion was the most prominent symptom in our patient. Pulmonary edema was also present but obstruction at the mitral valve orifice was not present. Most etiologies of pulmonary hypertension were chronic obstructive lung disease, pulmonary thromboembolism, mitral stenosis. Especially, reversible pulmonary hypertension was usually case of mitral stenosis, pulmonary thromboembolism. But pulmonary hypertension that revealed primary cardiac myxoma was rare.
Nakano et al.6) described positive correlation between the size of tumor and pulmonary artery pressure. The New York Heart Association function class and mean pulmonary artery pressure were decreased after tumor resection.
In our case, severe pulmonary hypertension was caused by large left side myxoma. After surgical removal, severe pulmonary hypertension and symptom were decreased.





 XML Download
XML Download