

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Ventricular septal defect (VSD) accounts for 20% of the congenital cardiovascular malformations and 10% of those VSDs diagnosed in adults. The vast majority of VSDs (roughly 70%) are located in the area of the membranous septum and they are defined as being perimembranous or subarterial. With a relative high incidence in Asian countries,1) the association of the subarterial type VSD with aortic valve prolapse (AVP), and mainly right coronary cusp prolapse, and aortic regurgitation (AR) has been shown. According to the previous reports, the incidence of AVP in the subarterial VSD was 36% to 79%.2)3) The peak age for AVP is around 7 years, and that for AR is between 5 and 10 years.3)4) VSD is a very common congenital heart defect in children, but due to spontaneous and surgical closure, it is less commonly encountered in adults.
When VSD is found in adult, about one-third of patents with VSD initially managed medically required surgical intervention later in life.5-7) In a tertiary referral population, there was an report that 25% of patients with small VSDs had serious complications, such as AR and endocarditis; these were the most common indications for surgical VSD closure in adults.6) Many experiences published case reports about surgical repair of AR complicating VSD in adolescents or young adults patients.5-7) But old adult patient was little known.
Here we reported a case of AR in a patient with right coronary cusp prolapse that was complicating a subarterial type VSD and the patient was 48 years old. It was diagnosed by thorough echocardiographic assessment and the patient underwent successful surgical closure of the VSD along with aortic valvuloplasty.
Case
A 48-year-old male visited emergency department due to retrosternal chest pain at rest for 6 hours and dyspnea on exertion for 3 months. He had been diagnosed with hypertension a year previously, but he had not taken any medication. He was a current smoker with 30 pack-years history and he drank alcohol daily. However, he had no medical history of arrhythmias, diabetes mellitus, ischemic heart disease or stroke. On arrival in the emergency department, his blood pressure was 150/90 mm Hg, his pulse rate was 100 bpm, his respiratory rate was 18 breaths per minute and his body temperature was 36.5℃. Cardiac auscultation revealed regular heart sounds with a pansystolic murmur and the lung sounds were clear. The initial electrocardiogram showed normal sinus rhythm and the chest radiography demonstrated a normal sized heart. The laboratory studies were within the normal limits.
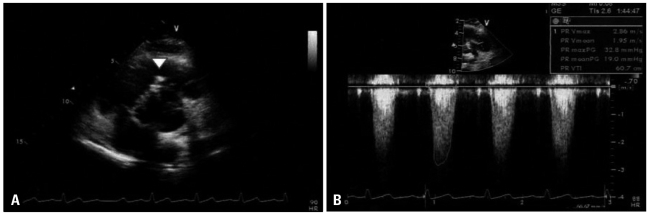
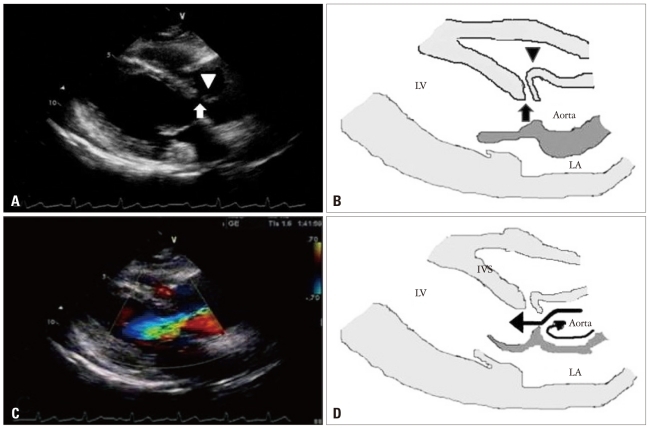
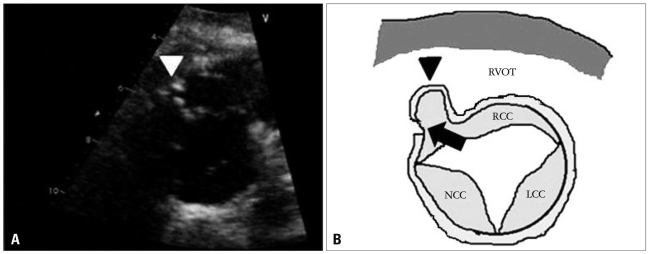
The initial transthoracic echocardiogram (TTE) revealed mild right ventricular outflow obstruction resembling subpul monic stenosis (Fig. 1), a subarterial type VSD of 4.2 mm diameter with left to right shunt flow (Qp/Qs = 2.01) and pressure gradient corresponding to 136 mm Hg. The right ventricular systolic pressure was 69 mm Hg and right ventricle was mildly hypertrophic. In parasternal long-axis view of TTE, the high velocity jet produced by the left-to-right shunt, through the VSD, results in a Venturi effect, displacing the unsupported annulus outward into the right ventricle (Fig. 2A and B). There was severe AR (Fig. 2C and D) with subtle right coronary cusp prolapse which caused mild right ventricular outflow obstruction. Also, in parasternal short-axis view at aortic level of TTE, there was right ventricular outflow tract obstruction due to right coronary cusp (RCC) driven into the right ventricle by high velocity left-to-right shunt flow (Fig. 3A and B).
Cardiac catheterization revealed that Qp/Qs and mean pulmonary artery pressure were measured as 1.41 and 19 mm Hg, respectively. Coronary angiography showed no significant luminal narrowing in coronary arteries.
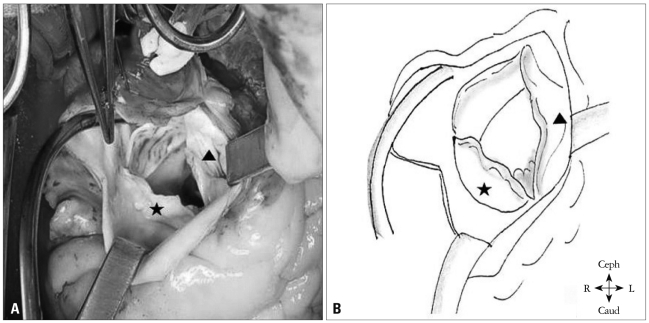
Although the Qp/Qs was low, we decided to perform an operation because he had dyspnea and severe AR. The surgical findings showed a prolapsed and retracted RCC and commissural calcification between the RCC and the noncoronary cusp (NCC). The VSD was nearly closed by the RCC (Fig. 4). He underwent surgical VSD closure with autopericardium through a pulmonary arteriotomy, and RCC mobilization with decalcification and commissurotomy between the RCC and the NCC. The post-operative course was uneventful. Post-operative TTE was performed and this revealed no residual shunt and only mild AR. In follow-up (after 48 months) examination, he had no symptom, and there was no specific change in follow-up TTE.
Discussion
In this report, we present a case of complicated VSD with severe AR due to right coronary cusp prolapse resembling subpulmonic stenosis in the relatively old adult. Although the patient's complicated VSD was diagnosed later in life, he was successfully treated with surgical repair after thorough echocardiographic assessment.
Echocardiography is the noninvasive method of choice for evaluating a VSD. It is a sensitive, descriptive tool with an excellent detection rate (88% to 95%), depending on the size and location of the defect and the technician's experience.8)9)
Thorough echocardiographic examination is best achieved by imaging the interventricular septum in multiple planes using color flow and spectral Doppler echocardiography. Echocardiography is most sensitive for defects larger than 5 mm and that are located in the membranous, inlet or outlet portion of the septum. It is least sensitive for detecting apical muscular defects. Echocardiography can confidently identify the morphologic features of the defect, including its size and borders and any associated defects.10)11) It also provides accurate hemodynamic assessment of the shunt and its severity, the volume overload, a subpulmonic (double-chambered right ventricle) or pulmonic stenosis, and pulmonary hypertension.12) In addition, echocardiography can assess the degree of aortic valve distortion and prolapse (the right and noncoronary cusps) in patients with a subarterial VSD and it can evaluate the severity of AR and right ventricular outflow tract obstruction caused by the prolapsing coronary cusp.13) Yearly echocardiographic assessment of AR has important prognostic implications, and especially with regard to the timing of surgical treatment. The mechanism of AVP in patients with subarterial VSD may include a lack of infundibular septal support, intrinsic discontinuity of the aortic valve annulus and aortic media, and a Venturi effect of the VSD jet.4)
The risk for AVP and regurgitation in patients with membranous or subarterial defects increases with age.14)15) AR is believed to be 2.5 times more frequent in patients with subarterial VSDs. Momma et al.15) reported on 395 patients with subarterial defects: AR was seen in 50% of the patients by 8 years and in 87% of the patients by 20 years. As the AVP progresses, the intraventricular shunting decreases at the expense of aortic valve distortion and regurgitation. This increases the risk for endocarditis, left ventricular volume overload, and less commonly, right ventricular outflow tract obstruction and sinus of Valsalva aneurysm.16)17) The progressive nature of the AR and the associated increased morbidity have led to recommending early surgical intervention.18)19) However, unless endocarditis supervenes, the rate of progression is often slow and variable. Therefore, the proper timing and type of operation are still controversial. The treatment of an isolated VSD depends on the type of defect, its size, the shunt's severity, the pulmonary vascular resistance, the functional capacity and the associated acquired anomalies, such as AR, subpulmonic stenosis, or pulmonary hypertension.20)21) Surgical closure of a VSD in adult decreases the risk for endocarditis by at least 50%, it reduces the pulmonary artery pressure, it improves the functional classification.21)22) and it can be accomplished with very low short- and long-term mortality and morbidity.23)
The case gives us two important lessons. The first, RCC or NCC prolapse should be suspected in AR complicating VSD through proper echocardiographic assessment. The second lesson was surgical repair of complicated VSD provides good result to the old adult patient, as well as the young.
 XML Download
XML Download