

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Double aortic arch (DAA) is a congenital anomaly, which is formed from the dividing of the ascending aorta into two limbs that pass around the trachea and esophagus, then enter a single descending aorta.1)2) In most cases, this anomaly can be diagnosed during infancy or childhood due to symptoms caused by esophageal or tracheal obstruction. For this reason, case reports of adults, especially asymptomatic cases, are rare.3) We report the case of a 36-year-old male with balanced type DAA, diagnosed coincidentally by echocardiography on a health check up.
Case
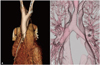
A 36-year-old man was admitted to our hospital for health check-up. The patient had no medical and family history of cardiac disease. Besides, the patient reported no medical abnormality in vital signs, physical examination, and laboratory findings. Chest radiography showed bilateral aortic notches at the level of aortic arch, suggesting aortic arch anomaly (Fig. 1). Two aortic arches on suprasternal view were seen on transthoracic echocardiography (Fig. 2). The diameter of the right aortic arch was 1.86 × 1.93 cm, while the left aortic arch was 1.46 × 1.51 cm in size. Multidetector computed tomography (CT) showed nearly same sized DAA forming a complete vascular ring encircling the trachea and esophagus. The right aortic arch was slightly larger and higher than the left aortic arch (Fig. 3). The esophagus had no compression within the vascular ring, while the trachea was slightly compressed by the vascular ring (Fig. 4).
The patient had no abnormal breathing sound and any other symptoms associated with compression of trachea or esophagus such as dyspnea, cough, dysphagia, and regurgitation. To evaluate the effect of the tracheal compression, pulmonary function test was done and showed normal findings. The patient was discharged from hospital with instructions for periodic follow-up.
Discussion
DAA is reported to be found in less than 1% of the congenital heart disease.4) In DAA, both the aortic arches form a complete vascular ring encircling the trachea and esophagus due to failure of regression of the right aortic arch.5)6) Each aortic arch passes the ipsilateral mainstem bronchus superiorly and enters the descending aorta, which is more commonly located on the left side than on the right side of the spine. Both aortic arches are often different in size and position. The right aortic arch is usually larger and located higher than the left aortic arch.7) The left aortic arch may be degenerated and so become atretic or remain as a fibrous band.8) The left and right common carotid and subclavian arteries come from each of the aortic arches.9) In our case, both aortic arches fuse into descending aorta located in front of the spine and the right aortic arch was slightly larger and located higher than the left aortic arch.
Classically, DAA is classified into three types depending on the relative size of the two arches and partial atresia of one arch; right dominant aortic arch, left dominant aortic arch, and balanced type aortic arch. Seventy-five percent of the DAA patients have right dominant aortic arch, and 20% have left dominant aortic arch. The dominance of either arch cannot be determined in the remaining 5%, called balanced type DAA. Accompanying intracardiac defect may be found in about 20% of the DAA patients.10-13) Our study patient had a balanced type of DAA. Although the right aortic arch was slightly larger than the left aortic arch, we could assume both aortic arches were nearly the same size and had no atresia of arch.
DAA patients may complain of respiratory symptoms or gastrointestinal symptoms caused by vascular ring formation. If the vascular ring compresses the trachea, the respiratory symptoms such as noisy breathing, dyspnea, cough, recurrent respiratory infections, apnea and cyanosis, which appear especially in neonates, could occur. Gastrointestinal symptoms such as feeding difficulty, emesis, and failure to thrive occur by esophageal compression.6) Symptoms can appear later in life when aorta enlarges due to atherosclerotic change.14) Our patients had no symptoms as mentioned above and normal findings in pulmonary function test in spite of slight compression of the trachea.
Chest radiographic features of the DAA patients include a deviation or compression of the trachea, or identification of a right aortic arch contour.15) We could see not only left aortic notch but also right aortic notch formed by right aortic arch in chest radiography of our patient.
Transthoracic echocardiography of the DAA patients can reveal aortic bifurcation on the subcostal view and the two descending aortic flow patterns on the suprasternal view.15)16) The echocardiography of our patient showed descending aorta, located in the middle, posterior to left atrium on parasternal short axis view and DAA on suprasternal view.
Some study reports that delineation of aortic arch abnormalities is difficult by conventional 2-dimensional echocardiography hence CT or magnetic resonance imaging (MRI) has been the diagnostic tool of choice.17) The transthoracic echocardiography in diagnosis of DAA patients has limited ability to image clearly the atretic aortic arch structures and ligamentum arteriosum. However, echocardiography remains a powerful, useful, non-invasive, and easily available modality which enables complete and accurate anatomic delineation and the exclusion of other major intracardiac defects.15)18)19)
The exact anatomy and location of an aortic arch malformation and adjacent structures can be accurately defined by CT and MRI, which allow 3 dimensional display of the malformations.9) The CT imaging of our patient revealed balanced type DAA resulting in only slight compression of the trachea and no compression of the esophagus.
A surgical approach is the only choice for the symptomatic DAA patients. Surgical intervention with division of the minor arch is recommended for those adult patients who are symptomatic and can be approached via either left posterolateral thoracotomy or median sternotomy.4)20)21) Because our patient had no symptoms, we did not perform any surgical intervention, however, we explained possible complications of DAA to the patient and recommended periodic follow-up.
In conclusion, balanced-type DAA is a rare condition. We report the case of a 36-year-old male with balanced-type DAA, diagnosed coincidentally by echocardiography on a health check up.



 XML Download
XML Download