

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Double-chambered right ventricle (DCRV) is a cardiac disease of the right ventricular outflow tract, where anomalous muscle bundles or a fibrous band cause obstruction.1-3)
A malaligned interventricular septal wall can develop in patients with aneurismal changes of ventricular septal defect (VSD), the degree of which usually increases with time.4) Furthermore, when combined with DCRV, VSD with malalignment between the outlet and trabecular septa was associated with tetralogy of Fallot. A subaortic ridge in the malalignment-type VSD is caused by turbulent flow.5-7) We describe here in the unusual case of a 56-year-old man who had a spontaneously healed membranous type VSD with malaligned interventricular septal wall, DCRV, subaortic ridge, and survived with surgical treatment.
Case
A 56-year-old male presented with resting dyspnea and chest discomfort for several years. He had no history of any surgical or catheter-based cardiovascular interventions. Physical examination showed a cardiac systolic murmur (grade 4/6) on the left upper sternal border, a systemic blood pressure of 140/75 mmHg, and a heart rate of 110 bpm. Electrocardiography showed sinus tachycardia, right axis deviation and frequent premature ventricular contraction with right ventricular bundle branch block morphology.
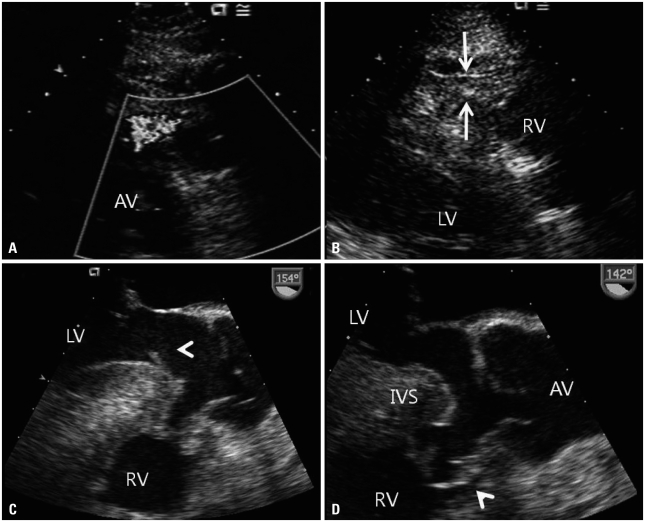
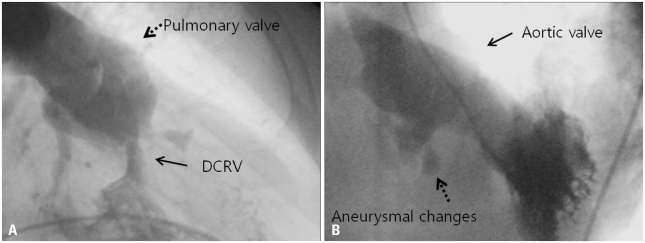
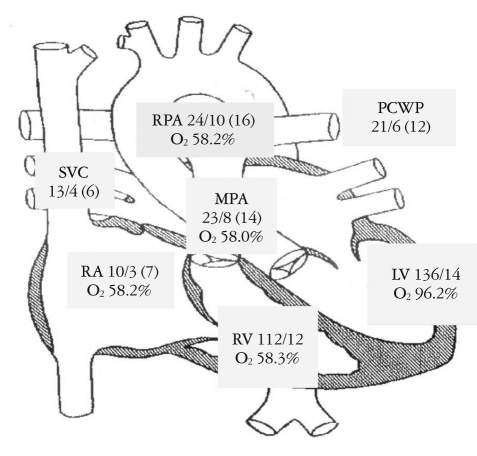
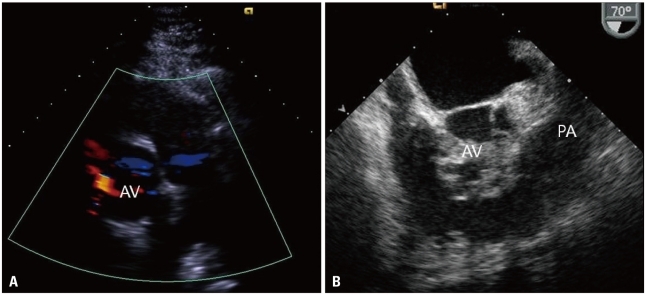
Transthoracic and transesophageal echocardiography revealed a membranous type VSD with anteriorly malaligned interventricular septum, aneurysmal changes, subaortic ridge and DCRV with right ventricular hypertrophy (Fig. 1). Measurement of pressure gradients using a Doppler image was not made because the ultrasound beam could not be made parallel to the outflow tract jet. Right ventriculography confirmed an anomalous obstruction within the right ventricle. Preoperative cardiac catheterization demonstrated a right ventricle-to-pulmonary artery gradient of 89 mmHg (Fig. 2 and 3). Left ventriculography revealed a membranous VSD with anteriorly malaligned interventricular septum, aneurysmal changes. The patient underwent open-heart surgery involving resection of an encircling infundibular fibrous band through right atriotomy. Resection of the subaortic ridge was not carried out because it caused mild aortic regurgitation without pressure gradients in the left ventricular outflow tract. Dyspnea was improved at follow-up. Transthoracic echocardiography taken after surgery revealed that the high-velocity systolic jet in the mid right ventricular outflow tract disappeared and that right ventricular outflow tract diameter was much improved (Fig. 4).
Discussion
Approximately two-thirds of patients have VSD that is diminished in size by aneurysmal changes with apposition of tricuspid tissue over the VSD.4) In our case, transthoracic and transesophageal echocardiography revealed a membranous type VSD with anteriorly malaligned interventricular septum, aneurysmal changes. The parasternal long axis view is useful for determining the degree of aortic overriding (Fig. 1D). DCRV is an infundibular pulmonary stenosis resulting from discrete fibromuscular narrowing or hypertrophied subvalvular muscle bundles. In many cases, VSD is combined DCRV.1-3) Also, malaligned between the outlet and trabecular septa VSD with DCRV is associated with TOF.6)8)9) In our patient, DCRV was not associated TOF because anteriorly malaligned interventicular septum without malalignment of infudibular septum was combined. VSD was located very close to the right aortic cusp and showed spontaneous closure with aneurysmal formation, which is rare without aortic valve prolapse.9-11)
The subaortic ridge is a fibrous structure from the crest of the ventricular septum to the left ventricular outflow tract. This case had a subaortic ridge caused by increased turbulence adjacent to the area of VSD and enhanced by septal malalignment.6)7) A subaortic ridge may result in progressive subaortic stenosis or aortic valve deformities, and resection is usually recommended. In our case, the patient underwent resection of an encircling infundibular fibrous band through right atriotomy. However, resection of the subaortic ridge was not carried out because it caused mild aortic regurgitation without any pressure gradients in the left ventricular outflow tract.
In summary, the malaligned interventricular septum in membranous type VSD can develop secondary to aneurismal changes of VSD. We reported the unusual case of a patient who had a pathology complex comprising DCRV, subaortic ridge, and VSD with malaligned interventricular septal wall and survived with surgical treatment.
 XML Download
XML Download