

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Metabolic syndrome (MS) is becoming a major health concern particularly in developed countries, with a prevalence of over 20% of the general adult population in the United States.1) Several studies from South Korea have reported that, as in Western countries, the prevalence of MS in the general adult population approximates 20%.2)3) MS is a known risk factor for the development of various cardiovascular diseases, including heart failure.4-8) Recent studies have shown that MS is directly related to relative left ventricular hypertrophy (LVH) and to systolic or diastolic dysfunction when assessed by two-dimensional or Doppler echocardiography.9-13) However, because in most of those studies, majority of patients had underlying diabetes mellitus (DM) or hypertension (HT), the influence of early MS on myocardial function has not been thoroughly evaluated. In addition, past studies have usually assessed diastolic function in MS patients by conventional Doppler echocardiography. Thus, we conducted this study to evaluate myocardial function in non-hypertensive MS patients by tissue Doppler Imaging (TDI) as well as conventional Doppler.
Methods
Study population
We screened subjects who visited the Healthcare Service Center of the Dong-A University Hospital. Complete cardiovascular examinations, including history taking, physical examination, and blood chemistry sampling, were performed in the outpatient clinic to screen for MS. Patients with known cardiovascular disease, HT, or stroke were excluded during the baseline examination. Weight, height, and waist circumference were obtained. Blood pressure (BP) was determined in the outpatient clinic using the conventional cuff method. Fasting serum glucose (FSG), total cholesterol, triglyceride (TG), high-density lipoprotein (HDL), and low-density lipoprotein levels were measured after fasting 12 hours overnight. For patients who were diagnosed with MS and agreed to participate in this study, signed informed consent was obtained, and comprehensive 2D and Doppler echocardiography were performed. We also selected control subjects who did not have MS. We applied the 2005 National Cholesterol Education Program (NCEP)/Adult Treatment Panel (ATP) III criteria to define MS. Subjects were diagnosed as having MS if they met three or more of the following criteria: waist circumference of ≥ 90 cm in men and ≥ 80 cm in women according to the NCEP/ATP III recommendations for the Asian population, TG level ≥ 150 mg/dL, serum HDL cholesterol level < 40 mg/dL in men and < 50 mg/dL in women, systolic blood pressure (SBP) ≥ 130 mmHg or diastolic blood pressure (DBP) ≥ 85 mmHg, and FSG level ≥ 100 mg/dL.14) However, patients with HT (systolic BP ≥ 140 mmHg or diastolic BP ≥ 90 mmHg by the Joint National Committee 7th report criteria)15) or DM (FSG level ≥ 126 mg/dL by the American Diabetes Association)16) were excluded for the purpose of this study. Patients who had systolic dysfunction, cardiomyopathy, or significant valvular heart disease on 2D echocardiography were also excluded. Being overweight or obese was defined as having a body mass index (BMI) between 25-29.9 kg/m2 or ≥ 30 kg/m2, respectively, according to the World Health Organization criteria.17) For this study, impaired glucose metabolism was defined as a FSG level of 100-125.9 mg/dL. Finally, we selected 42 consecutive MS patients without HT and 20 age-matched control individuals without MS.
Echocardiography
Echocardiography was performed using the iE33 ultrasound system and 2.5 MHz transducers (Philips Ultrasound Company, Cleveland, OH, USA). Standard parasternal and apical views were acquired. Complete 2D and M-mode echocardiogram, conventional Doppler, and TDI were obtained for all enrolled individuals. We measured the following left ventricle (LV) parameters by M-mode echocardiography: interventricular septal wall thickness (IVS), posterior wall thickness (PW), and LV end diastolic dimension (EDD) at the chordae tendinae level. The LV mass was calculated according to the following equation: LV mass = 0.8 [1.04 × (PW + IVS + LVEDD)3 - (LVEDD)3] + 0.6.18)
LV mass index was calculated as the LV mass divided by body surface area. LVH was defined as LV mass index ≥ 116 g/m2 for men and ≥ 104 for women.19) LV ejection fraction was measured by the modified Simpson method.20) Left atrial (LA) volumes were calculated using biplane Simpson method. LV diastolic function was evaluated by the measurements of early diastolic mitral inflow (E) velocity, late diastolic mitral inflow (A) velocity, E/A ratio, and mitral E wave deceleration time (DT) using conventional pulsed wave Doppler echocardiography. LV diastolic function was also estimated by TDI. Early diastolic mitral annular (Ea) velocity was measured by tissue Doppler placing sample volume at the lateral annulus.21)
To obtain longitudinal myocardial velocity, strain rate, and strain images with high quality, a narrow sector angle was used, and image depth was adjusted to allow for a high frame rate (> 120 frames/s) with care taken to avoid angulations. The myocardial time-velocity and time-deformation curves were reconstructed off-line from color coded 2D tissue Doppler image loops. The peak systolic (Sm), early diastolic (Em), and late diastolic longitudinal myocardial velocities were measured at basal and mid segments of the septal, lateral, inferior, and anterior walls from apical 2- and 4-chamber views. Likewise, peak systolic (Ssr), early diastolic (Esr), late diastolic strain rate, and peak systolic strain (PSS) were measured at the same segments and expressed as absolute values. Their average values were used to compare regional and global LV functions of MS patients to those of control subjects. A single investigator who was blinded to clinical data performed echocardiographic measurements.
Statistical analyses
Statistical analyses were performed using the Statistical Package for Social Sciences version 12 (SPSS Inc., Chicago, IL, USA). Continuous values were presented as mean ± standard deviations. Group means were compared using independent t-tests. Proportional values of the two groups were compared using Pearson's Chi-Square test. Pearson's correlation analyses were performed to assess the associations between clinical parameters of MS (age, waist circumference, SBP, DBP, TG, HDL, and FSG) and echocardiographic parameters of myocardial function (tissue Doppler myocardial velocity, strain rate, and strain). Multiple stepwise regression analyses were performed to evaluate the influence of clinical factors on the differences in echocardiographic findings. A p-value of less than 0.05 was regarded as having statistical significance.
Results
Study population
Demographic and clinical characteristics of the study populations (metabolic and non-metabolic control groups) are summarized in Table 1. Age and gender distributions were similar in both groups. Although there was no significant difference in BMI, waist circumference was significantly larger in the MS than in the control group. Another remarkable variation was demonstrated in terms of BP and TG levels between the two groups. The FSG and HDL levels were not significantly different between the two groups. Thus, MS patients included in the present study had minimal risk factors for MS.
M-mode, two-dimensional, and conventional doppler echocardiography
M-mode, 2D, and conventional Doppler echocardiographic measurements are shown in Table 2. LV size, LV mass, LA size, and LVEF were not significantly different between the two groups. LV diastolic function estimated by conventional Doppler criteria was similar in both groups. Thus, there were no significant differences in the prevalence of systolic and diastolic dysfunction when assessed by 2D and conventional Doppler echocardiography.
Tissue doppler imaging
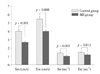
Echocardiographic measurements by TDI are summarized in Table 3 and Fig. 1. Tissue Doppler velocities of the lateral annulus were 8.8 ± 2.4 and 11.8 ± 1.9 cm/s (p < 0.001) in the MS and control groups, respectively. Average values of Sm and Em measured at 8 myocardial segments were significantly lower in the MS group than in the control group (2.7 ± 0.4 vs. 4.0 ± 1.0 cm/s, p < 0.001; 4.0 ± 1.3 vs. 5.5 ± 1.4 cm/s, p = 0.008, respectively). In addition, average values of Ssr, Esr, and PSS were also significantly lower in the MS group than in the control group (1.1 ± 0.3 vs. 1.4 ± 0.3 s-1, p = 0.001; 1.2 ± 0.3 vs. 1.5 ± 0.3 s-1, p = 0.013; and 16.9 ± 3.7 vs. 20.5 ± 3.2%, p = 0.001, respectively).
Relationship of clinical and echocardiographic parameters
Linear regression analysis was performed to examine the relationship of echocardiographic measurements to clinical parameters in patients with MS and non-MS (Table 4). Age significantly correlated with all echocardiographic parameters representing myocardial function. Waist circumference, SBP, and FSG had significant correlations with two of five echocardiographic parameters. Among the echocardiographic parameters, Sm is the most representative paramenter which is able to evaluate myocardial dysfunction in MS in present study. A correlation index of Sm greater than 0.3 was seen in waist circumference and SBP.
TG and HDL levels did not have significant correlations with any of the echocardiographic parameters. Stepwise multiple regression analysis was performed to examine the clinical parameters that influence global Sm (Table 5). The results indicated that age (β coefficient = -0.313, p = 0.006), waist circumference (β coefficient = -0.296, p = 0.012), and SBP (β coefficient = -0.253, p = 0.031) were independently associated with Sm.
Discussion
The results of our study showed that non-hypertensive MS patients had subclinical myocardial dysfunction that was made apparent by TDI.
Previous studies have shown echocardiographic evidence of myocardial dysfunction in MS patients.11)12) However, most patients enrolled in those studies had overt DM or HT. Thus, diastolic dysfunction was evident by conventional parameters (E, A, and E/A) as well as TDI indices. In contrast, the present study shows that myocardial dysfunction in patients with an early stage of MS was detected by TDI not conventional parameters. We designed this study to test the hypothesis that early MS patients might have myocardial dysfunction. We excluded HT patients to estimate the true impact of early stage MS on myocardial function, which was the most important aspect of the present study. In addition, a study of MS patients without DM or HT lends itself to a better examination of the relationship between each metabolic parameter to myocardial function, because HT by itself is strong enough to cause a decline in diastolic function.
Peak longitudinal myocardial velocities derived from pulsed wave TDI are useful indicators of global or regional LV dysfunction. The early diastolic TDI velocity of the mitral annulus is generally thought to be a preload independent index for LV relaxation, and it is used to estimate LV filling pressures.22)23) Strain and strain rate are other tools that can reflect myocardial function.24)25) We applied tissue Doppler myocardial velocity, strain, and strain rate together to detect subtle changes in global myocardial function.
Conventional Doppler echocardiography revealed a tendency for MS patients to have more diastolic LV dysfunction. However, that tendency did not achieve statistical significance. In contrast, TDI studies showed significant differences that were not revealed by conventional pulsed wave Doppler studies. Lateral Ea velocity, Sm, Em, Ssr, Esr, and PSS were more profoundly decreased in the MS group compared to control, and the differences achieved statistical significance. The results of our study suggest that TDI is superior to a conventional pulsed wave Doppler study in detecting early myocardial dysfunction.
The 34 patients with MS enrolled in our study were diagnosed by 3 criteria: waist circumference, low HDL levels, and high TG levels. Waist circumference reflects central obesity and risk of cardiovascular disease. Furthermore, it is considered to be the best predictor of MS among other diagnostic criteria.26) On the other hand, the direct influence of dyslipidemia on myocardial function is not well known. A recent study showed that short-term control of dyslipidemia using statin improved myocardial dysfunction assessed by the Tei index and tissue Doppler myocardial velocities. In that study, as in our current one, overt DM and HT patients were excluded; however, waist circumference was not measured. The results suggested that dyslipidemia itself may be a risk factor for myocardial dysfunction.27)
In this study, we expected that waist circumference and lipid levels would exhibit good correlations with echocardiographic parameters because most MS patients were diagnosed by waist circumference and dyslipidemia. However, all metabolic parameters had a weak correlation with echocardiographic indices. Especially, dyslipidemia itself was not related to echocardiographic parameters, because the patients enrolled in this study had mild abnormalities of lipid profile. These data are different from previous study.27) Based on our results, age was the best parameter to predict myocardial dysfunction. Of the metabolic parameters, waist circumference and SBP were more important than FSG, TG and HDL in influencing myocardial dysfunction in patients with early MS. From multiple comparisons of echocardiographic and metabolic parameters, the highest correlation was observed between age and Em (r = -0.551, p < 0.001); however, metabolic parameters were more closely related to Sm than Em. The data in the present study indicate that waist circumference and SBP are independently associated with myocardial dysfunction (Sm).
It is common knowledge that even a mild degree of diastolic dysfunction may be associated with poor prognosis on long-term follow-up;29) therefore, early detection of myocardial dysfunction may provide MS patients with a chance to modify their lifestyles, thereby preventing future heart disease. The use of TDI might detect early systolic and diastolic myocardial dysfunction in MS patients, even if they do not have overt DM, HT, or any structural abnormalities.
There are a few limitations in present study. Firstly, the size of this study to assess the relationship of each MS factor with myocardial dysfunction was relatively small. Secondly, it is difficult to explain the exact pathophysiologic mechanisms of how early MS without overt HT influences myocardial function, although we postulate that insulin resistance that was not measured in this study might underlie decreased myocardial function. Thirdly, although all subjects in our study did not have any signs or symptoms of angina, and had normal findings on electrocardiogram and on 2-D echocardiography, we could not completely exclude asymptomatic coronary artery disease.
In conclusion, these results indicate that patients with MS without HT may have myocardial dysfunction apparent by tissue Doppler imaging, even if they appear to have normal findings on two-dimensional and conventional Doppler studies.




 XML Download
XML Download