

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In the population-based studies, degenerative aortic valve diseases become notably more common, with an increasing prevalence in the population over age 65 years.1) An improved comprehension of the aortic root geometry could assist with better understanding the pathophysiology of aortic valve diseases, improving the diagnosis of aortic valve disease and further developing either surgical or transcatheter aortic valve implantation.
There is ambiguity about both the precise nature and the relationship between various structures composing the aortic root.2) However, there have been many attempts to understand the aortic root geometry.3-6) The volumetric approach of the aortic root geometry has never been attempted. The volumetric measurements might improve the knowledge about the aortic root geometry.
Three-dimensional (3D) echocardiography has been reported to be valuable for evaluating the geometry of cardiac chambers.7-9) We hypothesized that 3D transthoracic echocardiography (TTE) could be one of imaging modalities for volumetric quantification of the aortic root geometry. We evaluated the accuracy of 3D TTE for quantifying the aortic root geometry in comparison with cardiac multi-detector computed tomography (MDCT).
Methods
We retrospectively studied 23 consecutive patients who underwent cardiac MDCT and showed normal ejection fraction (> 55%), as assessed by two-dimensional (2D) TTE. The conventional 2D and 3D studies were performed within 1 month, either after or before undergoing cardiac MDCT. The medical records of all patients were retrospectively reviewed. We excluded from the study the patients with any of the following: valvular heart disease, cardiomyopathy, left ventricular hypertrophy and atrial fibrillation. In the literature, there is no published data on the volumetric assessment of the aortic root volume. Therefore, we excluded from our study the patients with any pathologic findings that could affect the aortic root geometry. This study was approved by the Institutional Review Board at Ajou University Hospital (approval number: AJIRB-MED-MDB-11-140).
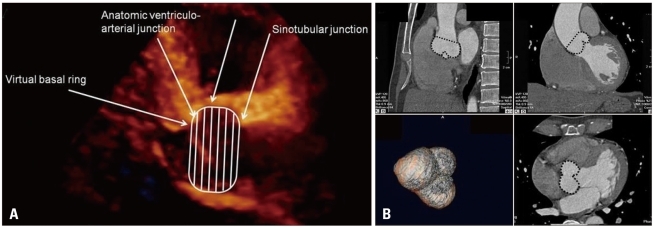
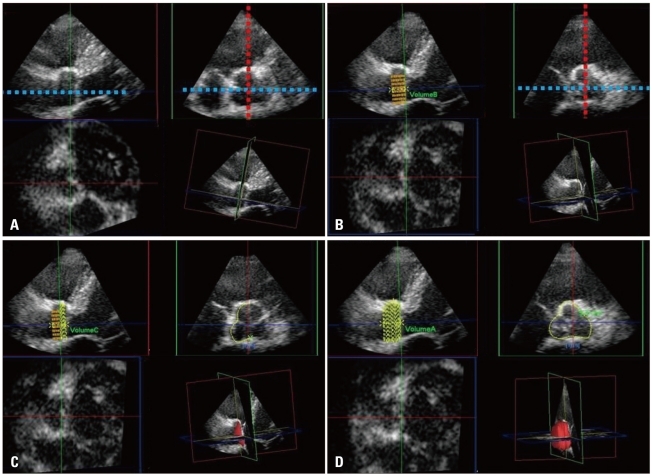
The study was conducted using the Philips iE33 ultrasound system and the X3-1 matrix-array transducer (Philips Medical Systems, Andover, MA, USA). A full volume loop was acquired from the parasternal long axis view over four cardiac cycles. Measurements of the 3D aortic root volume were performed offline by an experienced physician, using the QLAB Advanced Ultrasound Quantification Software Release 8.1 (Philips Medical Systems, Andover, MA, USA). We defined the aortic root volume as the volume from the aortic annulus to the sinotubular junction (Fig. 1). The multiplanar reconstructive method (MPR) was used for quantification of the aortic root geometry. One plane was aligned with the parallel line of the long axis of the ascending aorta, passing the coaptation point of the aortic cusps. A second line was set as the line perpendicular to the first line and cut across the coaptation point of the three aortic cusps. The stacked contour mode was used. The borders of the stacked contour were set from the aortic annulus to the sinotubular junction. From the aortic annulus to the sinotubular junction, twenty default slices were set. The aortic root was equally divided along the first line into 20 slices. Semi-automated border detection was performed to define the contour of each slice. For more accurate measurements, we corrected each contour manually. We traced the contour as the inner layer of the aortic root. After defining the contour of each slice, the volume was calculated automatically, using integration of each area (Fig. 2). The end-systolic aortic root volume was measured at the end of the T wave on electrocardiogram. The end-diastolic aortic root volume was measured at the starting point of the R wave on electrocardiogram. The left ventricular end-diastolic and end-systolic volumes and the ejection fraction were calculated in 2D TTE using the biplane modified Simpson's rule.
Sixty-four channel cardiac MDCT was performed with the Brilliance 190p (Philips, Eindhoven, Netherlands). The end-diastolic aortic root volumes were measured. Vitrea2 imaging software version 3.1 (Vital Images, Plymouth, MN, USA) was used for acquiring advanced 3D volume data of the aortic root. Due to limitation of the imaging acquisition protocol of MDCT, we could not record with MDCT any data of the end-systolic volume of the aortic root.
The SPSS 12.0 (SPSS Inc., Chicago, IL, USA) statistical software package was used for analysis of descriptive data. All descriptive data are expressed as mean ± standard deviations (SDs) for the continuous variables, and as percentages for the categorical variables. The end-diastolic aortic root volume determined by 3D TTE was compared with the end-diastolic aortic root volume calculated by MDCT. The linear association between the two methods was assessed with linear regression analysis and with Pearson's correlation coefficient. Bland-Altman plot was created to calculate the limits of agreement between the two methods.10)
Results
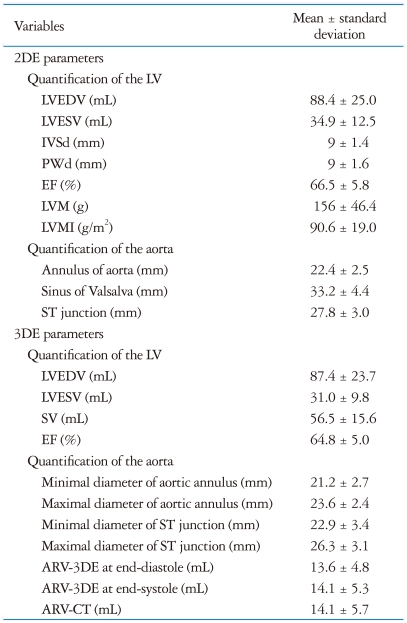
The study population consisted of 23 patients (mean age 53 ± 9 years, 12 male and 11 female). The 2D and 3D echocardiographic parameters of the study population are summarized in Table 1. There was no statistically significant difference in the left ventricular end-diastolic and end-systolic volumes and ejection fraction between 2D TTE and 3D TTE.
The cross-sectional area of the aortic root was asymmetric. At the level of the annulus, the cross-sectional area showed asymmetric triangle. From the aortic annulus to the most dilated point of the sinus of Valsalva, the asymmetric triangular shape was maintained. From the most dilated point of the sinus of Valsalva to the sinotubular junction, the cross-sectional shape of the aortic root changed to oval (Fig. 3). Mean difference between the maximal and minimal diameters of the annulus and the sinotubular junction were 2.4 ± 1.3 mm and 3.4 ± 1.9 mm, respectively, indicating asymmetry of aortic root (Table 1).
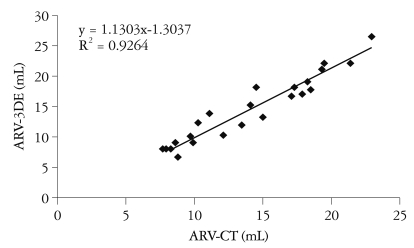
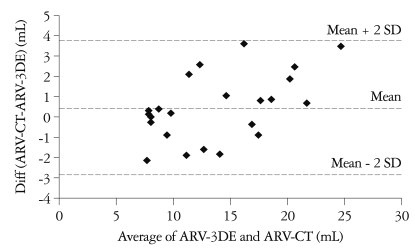
The aortic root volume measured by 3D TTE (ARV-3DE) at end-diastole was 13.6 ± 4.8 mL, and the aortic root volume measured by MDCT (ARV-CT) at end-diastole was 14.1 ± 5.7 mL. The end-systolic ARV-3DE was 14.1 ± 5.3 mL. By linear regression analysis, 3D TTE showed good correlation with MDCT in the assessment of the aortic root volume (R2 = 0.93) (Fig. 4). The ARV-3DE showed an excellent agreement with the ARV-CT (difference = 0.5 ± 1.7 mL, % difference = 0%) (Fig. 5). There was no statistically significant difference in the distance between the annulus and the ostium of the left coronary artery, the distance between the annulus and the ostium of the right coronary artery and the distance between the annulus and the sinus of Valsalva, which are known as useful parameters for the selection of candidates for transcatheter aortic valve implantation, between 3D TTE and MDCT (Table 2). By an experienced physician, measurements of the 3D aortic root volume, using the QLAB Advanced Ultrasound Quantification Software Release 8.1, took around 1 minute. The absolute values of the mean paired differences were 0.288 ± 0.2995, p = 0.794 and 0.522 ± 0.872, p = 0.11 for inter- and intra-observer variability of the aortic root volume measured by 3D TTE, indicating good reproducibility and feasibility.
Discussion
The present study demonstrated that 3D TTE could be used for quantification of aortic root volume. Also, we presented the new method for understanding the aortic root geometry.
Accurate assessment of the aortic root is considered as increasingly important. Two-dimensional echocardiography has had an important role in the assessment of the aortic root geometry. The dimensions of the aortic root can be measured with 2D echocardiography. There is ambiguity about both the precise nature and the relationship between the various structures composing the aortic root.2) Several studies demonstrated that the aortic root geometry was asymmetric.4)11)12) In the present study, we also demonstrated the asymmetry of the aortic root. Due to the asymmetric characteristics of the aortic root geometry, the 2D echocardiographic measurement of the aortic valve annulus may not be the ideal approach.13) The asymmetric aortic root geometry can be accurately visualized with 3D imaging techniques.4)13) Three-dimensional imaging techniques provide highly accurate measurements, by allowing proper orientation of the orthogonal multiplanar reformation planes through all the levels of the aortic root.
Cardiac magnetic resonance imaging (CMR) and cardiac MDCT are considered the gold standard imaging techniques to evaluate the aortic root.13) However, CMR is not widely available, is more costly, and cannot be used on patients with implanted pacemakers or defibrillators and cardiac MDCT involves radiation exposure. Therefore, 3D echocardiography might be more suitable for clinical practice. As CMR and cardiac MDCT still have limited temporal resolutions, compared with echocardiography, the 3D echocardiography is considered a promising imaging technique for accurate measurement of the aortic root geometry and for assessment of the aortic root dynamics. Many comparison studies between 3D echocardiography and either CMR or cardiac MDCT showed that 3D TTE was valuable for evaluating the geometry of cardiac chambers.7-9) In the present study, we validated the accuracy of 3D TTE for quantifying the aortic root geometry in comparison with cardiac MDCT.
For a true understanding of anatomic and pathologic structures, the interpretation of 2D echocardiographic images requires a complex mental integration of multiple planes. Three-dimensional echocardiography allows direct calculation of volumes and is more accurate and closer to the real world than 2D echocardiography, relying on geometric assumption.14) Three-dimensional volumetric quantification of the aortic root may also give information closer to reality than geometric assumption. Using MPR method, volumetric quantification of the aortic root is quite simple and accurate and may be easily applied in clinical settings.
There are several limitations to the present study. Firstly, using the MDCT, we could not record any data of the end-systolic volume of the aortic root, due to limitation of the imaging acquisition protocol. Thus, in the present study, we validated the aortic root volumetric quantification only at end-diastole. Second, we manually corrected the contour of the aortic root in this study, because the accuracy of automatic measurements was questionable in many cases. Manual correction may include the possibility of researcher bias. Further development of specialized software for automatic measurements might be needed for the accurate and feasible assessment of the aortic root volume. Third, we could not validate the volumetric measurements of the geometry of the aorta beyond the sinotubular junction. Since the aortic valve disease usually changes the geometry of the aorta, the accurate assessment of aorta geometry may also be necessary for understanding the aortic disease. Advancement of software, which could accurately measure both the volume and dynamics of the aorta, including the aortic root, would be necessary for the reliable clinical application of 3D TTE volumetric quantification in aortic valve disease. Fourth, we excluded from our study the patients with any pathologic findings that could affect the aortic root geometry. Therefore, the results of the study could not be applied to the whole population including the diseased population. A prospective study including the diseased population might be needed for clinical application of 3D echocardiographic quantification of aortic root geometry.
Our results demonstrated both the feasibility and the accuracy of 3D TTE for the volumetric assessment of aortic root geometry. The MPR method has been already validated for the assessment of the ejection fraction and LV volumes, and could be an effective tool for volumetric quantification of the aortic root. Thus, the volumetric assessment of the aortic root geometry by 3D TTE could be the new method for understanding the aortic root geometry.


 XML Download
XML Download