

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pheochromocytoma is a rare tumor derived from chromaffin cells of the adrenal gland. It can secrete excessive catecholamine and cause clinical problems.1)2) Stimulation of alpha-adrenergic receptors results in elevated blood pressure, increased cardiac contractility, glycogenolysis, gluconeogenesis, and intestinal relaxation. Stimulation of beta-adrenergic receptors results in an increase in heart rate and contractility. Excessive catecholamine release can cause transient reversible cardiomyopathy associated with pheochromocytoma.3)4) There are many sporadic case reports about transient episode of heart failure associated with pheochromocytoma. However, there is no known article about the incidence of cardiomyopathy in the patients with pheochromocytoma. Thus we evaluated the patterns of clinical presentation and the incidence of catecholamine cardiomyopathy in Korean patients with pheochromocytoma.
Methods
From January 2004 to April 2011, all consecutive patients with pheochromocytoma were enrolled retrospectively. Pheochromocytoma was diagnosed by histologic examination after surgical removal. We investigated their clinical symptoms, serum catecholamine profiles, urinary excretion of catecholamines and radiologic findings including computerized tomography (CT) with review of their medical records.
The patterns of electrocardiography and echocardiography were also analyzed. The electrocardiographic examinations were performed at the time of diagnosis. Electrocardiograms were interpreted independently without knowledge of the clinical or echocardiographic finding by a specialist (J.H.K). Echocardiographic examinations were carried at the time of diagnosis and surgical removal. Complete two-dimensional, M-mode and Doppler studies were performed using standard parasternal, apical, and subcostal approaches using Vivid 7 (GE Medical Systems, Waukesha, Wisconsin). End-diastolic and end-systolic LV volumes were measured in the apical four and two chamber view with a modified Simpson's method. The LV ejection fraction was subsequently calculated. Mitral inflow velocities were calculated with a pulsed wave Doppler at the tip of the mitral valve. Mitral annular velocities were measured with tissue Doppler imaging of the mitral annulus. The calculated LV ejection fraction of less than 50% was considered the presence of LV systolic dysfunction. If there was a LV systolic dysfunction, a follow-up echocardiography examination was done, repeatedly.
Blood test for plasma catecholamines was done by a liquid chromatographic method (epinephrine less 15 pg/mL, and norepinephrine less than 25 pg/mL are normal in our laboratory).5) Urinary catecholamines were measured by a liquid chromatographic method and expressed as µg/24 hours (norepinephrine less than 80 µg/24 hours, epinephrine less than 22 µg/24 hours, vanillylmandelic acid less than 8 mg/24 hours, and metanephrine less than 0.8 mg/24 hours are normal in our laboratory).5)6)
Results
During the study period, total 36 patients (21 males, 49.8 ± 15.8 years, range 14-81 years) with pheochromocytoma were enrolled. Their clinical characteristics were listed in Table 1. Most common presenting symptom was abdominal pain (36.1%). Nine (25.0%) of them had no clinical symptoms. Most common reason of detection of pheochromocytoma was routine screening (17, 47.2%). Others were evaluation of abdominal pain (8, 22.2%), dyspnea (4, 11.1%), hypertension (3, 8.3%), headache (3, 8.3%), and palpitation (1, 2.8%). Previous history of cardiovascular disease was rare. Cardiac risk factors were 47.2% with hypertension and 16.7% with diabetes. The serum glucose level was high (157.8 ± 70.5 mg/dL).
All patients underwent electrocardiographic examination. Normal finding was the most common (19, 52.8%). LV hypertrophy was found in 12 (33.3%), sinus tachycardia (> 100/min) in 3 (8.3%) and other findings (2 nonspecific ST segment change and 1 supraventricular tachycardia) in 5.6%. Because there was no clinical symptoms and electrocardiographic abnormality, echocardiographic exam was not done in 7 patients. Of total 29 patients, most common finding was normal LV systolic function in 18 patients. Majority of patients (22, 75.9%) underwent echocardiographic examination showed relaxation abnormality.
Three patients showed transient LV systolic dysfunction (2 with inverted Takotsubo type cardiomyopathy and 1 with diffuse hypokinesia pattern). Common presenting symptoms were new onset chest discomfort and dyspnea. However, there was no relationship between the presence of LV systolic dysfunction with tumor size or presence of necrosis in it. Their electrocardiographic examinations demonstrated sinus tachycardia without evidence of ST segment change. All three patients admitted to the emergency department and cared in the intensive care unit. Their clinical profiles were summarized in the Table 2.
Case 1
A 32-year-old man visited our emergency department with palpitation and squeezing chest pain. His initial blood pressure was 190/112 mmHg and electrocardiogram showed sinus tachycardia of 120/min. The initial electrocardiogram revealed slight ST-segment elevation in lead II, III, and aVF. Echocardiography demonstrated a midventricular dilatation of the LV and decreased LV ejection fraction of 35% (Fig. 1A and B). However, the motion of the LV apex was preserved. Serum levels of cardiac biomarkers were increased. The serum level of N-terminal-pro-B type natriuretic peptide (NT-pro-BNP) was increased up to 733.3 pg/mL (normal range: < 200 pg/mL). The coronary arteries were free of any organic stenosis and LV angiogram showed severe hypokinesia in the mid to basal portion with preserved LV apical wall motion. The serum and 24-hour urine studies were compatible with pheochromocytoma. An abdominal CT showed an approximately 7.8 × 8.3 × 10.0 cm large septated cystic mass with irregular wall enhancement of the right adrenal gland and scintigraphy scan with 123I-MIBG showed huge round uptake in the right adrenal gland. The patient was treated with oral furosemide, an oral alpha blocker and intravenous nitrate infusion. The low dose of beta blocker was initiated after alpha blockade. The follow up echocardiography after three days of treatment showed marked improvement of LV systolic function and decreased LV dimension. The LV ejection fraction was 59%, with no regional wall motion abnormalities (Fig. 1C and D).
Case 2
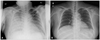
A 41-year old man presented to the emergency room due to new-onset dyspnea. His initial blood pressure was 180/100 mmHg and heart rate was 140/min. The initial electrocardiogram demonstrated sinus tachycardia. Chest radiography showed pulmonary edema which improved after 3 days (Fig. 2). Serum levels of cardiac biomarkers were increased. NT-pro-BNP was markedly increased up to 34,489 pg/mL. Echocardiography showed severe LV dysfunction and a contractile abnormality, consisting of akinesis of the basal and mid ventricular segments and hyperkinesis of the apical segments (Fig. 3A and B). The patient was admitted at intensive care unit and intravenous administration of dobutamine, furosemide, and digoxin. His symptoms were improved in one day despite of sporadic surge of blood pressure and pulse rate. The 24-hour urine study was compatible with pheochromocytoma. The abdominal CT revealed about 4.9 × 5.7 × 4.5 cm sized right adrenal cystic mass with hemorrhage. Follow up echocardiography, repeated after two days, demonstrated normalized LV systolic function and regional wall motion abnormalities (Fig. 3C and D). The elective laparoscopic right adrenalectomy was performed after 4 weeks of therapy including alpha and beta blockers.
Case 3
A 49-year-old woman with hypertension and diabetes mellitus was admitted to emergency room with dyspnea and chest discomfort. She complained palpitation and recurrent headache for several months. Her initial blood pressure was 160/114 mmHg and heart rate was 100/min. The initial electrocardiogram demonstrated sinus tachycardia. Chest radiography showed marked pulmonary edema (Fig. 4). Because the patient showed severe hypoxemia, she was intubated and cared with ventilator in the intensive care unit. Her condition improved dramatically after 1 day and ventilator was removed after 2 days. Cardiac enzymes were slightly elevated and NT-pro-BNP increased up to 2,458 pg/mL. Echocardiography showed severe LV systolic dysfunction with an estimated ejection fraction of 20% and severe hypokinesia of all segments. A 24-hour urinary catecholamine excretion was compatible with pheochromocytoma. Follow up echocardiography, repeated after two days, demonstrated normalized LV systolic function and regional wall motion abnormalities. Cardiac catheterization was performed and angiographically normal epicardial coronary arteries. The patient was hemodynamically stabilized with conventional treatment. The abdominal CT scan revealed about 3.3 × 6.2 sized tumor of the left adrenal gland and 131I-MIBG scintigraphy showed a hot-uptake lesion of the same location.
Discussion
The prevalence of catecholamine cardiomyopathy associated with pheochromocytoma is about 10% (3 of 29 patients) in our study. The patterns of cardiac involvement are 2 inverted-Takotsubo cardiomyopathies and 1 diffuse severe hypokinesia. All three patients showed complete recovery with inotropic support and conventional treatment within 3 days.
Pheochromocytomas are rare catecholamine producing tumors typically located in the adrenal gland or along the sympathetic ganglia. Due to secretion of catecholamines, they usually present with a classic triad of headache, tachycardia and sweating.7)
Shub et al.8) reported echocardiographic patterns in 26 patients with pheochromocytoma. In their data, most common echocardiographic finding was normal or increased systolic function (80% of the patients). The result of our study is consistent with this study. However, relaxation abnormality is the most common finding in our study (22, 75.8%). The increased incidence of diastolic dysfunction may be associated with injury of myocytes or increased oxidative stress by circulating catecholamines.9)10)
It has also been reported to cause cardiac manifestations including a transient, reversible cardiomyopathy (catecholamine cardiomyopathy).11) Shaw et al.11) firstly reported echocardiographic feature of catecholamine cardiomyopathy associated with pheochromocytoma in the late 1980s. It resembles Takotsubo cardiomyopathy (transient apical ballooning syndrome) presenting with hyperkinesis of the basal segments and apical hypokinesis.3)12-14) The LV systolic dysfunction usually recovers completely within several days. Proposed potential mechanisms of transient LV ballooning include micro-vascular dysfunction of the coronary arteries, multivessel epicardial spasm, impaired fatty acid metabolism, myocarditis and catecholamine-mediated myocardial dysfunction.15)16) Although the mechanism of the association between sympathetic stimulation and myocardial stunning is still unknown, several proposed mechanisms have been proposed including coronary arterial spasm17) and direct injury to myocytes.9) The apex is more vulnerable to a sudden increase in circulating catecholamine levels may be due to different distribution of sympathetic nerves18) and dissimilar density of sympathetic nerves in the heart.19) More recently, a variant of Takotsubo cardiomyopathy, the 'inverted-Takotsubo cardiomyopathy' has been described.15) It distinguished by dysfunction of the basal and mid-ventricular segments with preserved function of the apical segments. Cases of inverted-Takotsubo cardiomyopathy associated with pheochromocytoma were also reported.20-22) Two of our cases showed inverted-Takotsubo cardiomyopathy which recovered completely within 3 days. The variations in segmental involvement regardless of coronary anatomy in patients with excessive catecholamine levels may suggest different susceptibility to sympathetic stimulation from individual to individual.20)
Despite this study firstly described the prevalence of transient LV systolic dysfunction with echocardiographic examination, this study has many limitations. First, this study is a retrospective study with review of their medical records. The incidence and pattern of LV systolic dysfunction could not be assessed exactly. However, all three patients with LV systolic dysfunction complained new onset dyspnea and chest discomfort led to visiting emergent department. Their serum NT-Pro BNP levels were elevated and echocardiographic examination revealed the presence of LV systolic dysfunction. Moreover, 9 of total patients had no presenting symptoms suggesting presence of LV systolic dysfunction. Second, echocardiographic examination was not performed in all participants. Echocardiographic examination was not performed in the patients without clinical symptoms and with normal electrocardiographic findings (7, 19.4%). Pheochromocytoma is a very rare tumor and the detection is difficult especially without presenting symptoms. To evaluate the exact incidence and pattern of catecholamine cardiomyopathy associated with pheochromocytoma, prospective study will be needed.
In conclusion, of total 36 patients with pheochromocytoma, 3 showed transient LV systolic dysfunction (catecholamine cardiomyopathy associated with pheochromocytoma). Two of their echocardiographic patterns were inverted-Takotsubo cardiomyopathy and 1 was diffuse LV hypokinesia. Their echocardiographic abnormalities were normalized with conventional treatment within 3 days.





 XML Download
XML Download