

 PDF
PDF ePub
ePub Citation
Citation Print
Print


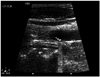
A 63-year-old male presented to the emergency department being shot with a hunting shotgun from a distance of more than 10 m. He had multiple entry wounds from pellets in the neck, thorax, abdomen, scrotum and upper extremities, with no exit wounds. He was haemodynamically stable and had a whole body CT scan with no intravenous contrast because of chronic renal insufficiency. A pellet adjacent to the left common carotid artery was demonstrated, accompanied by a limited hematoma. Additionally, a pellet was shown next to the trachea, and multiple pellets throughout his torso. Carotid Duplex demonstrated a pellet embedded in the posterior-medial wall of the left common carotid artery, producing a focal intraluminal protrusion of the intima with no tear (Fig. 1). Bronchoscopy was normal. Repeat duplex and bronchoscopy after 48 hours did not show any change. Clopidogrel 75 mg once daily was prescribed and he was discharged after five days. At six months the patient was asymptomatic and repeat Duplex showed no interval changes.
Retained intramural pellet has not been previously reported for the carotids. Additionally, no retained intramural missiles or foreign bodies elsewhere in the cardiovascular system have been reported except for the myocardium. There is lack of data regarding the natural history of such a carotid pellet, but the experience from the myocardium is that, in the absence of infection, completely embedded missiles are usually asymptomatic, tolerated well and may be left in place.1) It is prudent for our patient to be on a life-long follow-up with duplex ultrasound in order to reveal possible complications like dissection, erosion and pseudoaneurysm or arteriovenous fistula formation. Another possible late complication could be intimal erosion and pellet migration to intracranial circulation, as has been previously described in acute cases.2) Lead toxicity, another well-recognized late complication can occur months to years after the event.3)
 XML Download
XML Download