

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Stress-induced cardiomyopathy (also known as takotsubo cardiomyopathy or apical ballooning syndrome) is characterized by acute, reversible and transient left ventricular (LV) systolic dysfunction that resembles acute coronary syndrome but does not show significant stenosis on coronary angiography.1)2) Emotional and/or physical stressor can be the triggering factor. Excessive release of catecholamines due to stressors has been proposed to be involved in the pathogenesis of stress-induced cardiomyopathy because it causes structural changes of LV and disturbances in Ca2+ homeostasis.3) The recent body of evidence shows that postmenopausal women (90%) are predominantly affected by this syndrome and that stress-induced cardiomyopathy comprises 0.7-2.5% of cases of myocardial infarction (MI).4-6) Approximately 20% of complications were reported, including cardiogenic shock, heart failure, arrhythmias, intraventricular thrombus formation, LV free wall rupture, and even death.1)3)4)
Easy accessibility at the bedside of the hospitalized patient and the ability to use real-time noninvasive hemodynamic evaluation are the distinctive characteristics of echocardiography, particularly in the emergency setting. This review primarily addresses the role of echocardiography and emphasizes its usefulness in the diagnosis and management of this challenging disease.
Definition and Diagnosis
The criteria for the diagnosis of stress-induced cardiomyopathy have evolved over the years. The most recently available criteria were proposed by the Mayo Clinic in 2008.7) The modified version of these criteria consists of four components: A) transient hypokinesis, akinesis, or dyskinesis in LV mid-segments with or without apical involvement; abnormalities in regional wall motion extending beyond a single epicardial vascular distribution; the presence (often, but not always) of a stress trigger; B) the absence of obstructive coronary disease or angiographic evidence of acute rupture of plaques that could be responsible for the observed wall motion abnormalities; C) new electrocardiographic abnormalities (ST-segment elevation and/or T-wave inversion) or modest elevation of levels of cardiac troponin in serum; and D) the absence of pheochromocytoma or myocarditis.
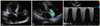
For the diagnosis of stress-induced cardiomyopathy, echocardiography is the most important imaging modality to distinguish this syndrome from acute MI, although coronary angiography is the best single tool to diagnose this unique cardiomyopathy. Abnormalities in LV wall motion show a regional or global pattern with a relative hypercontractile base in most cases. An inverted takotsubo pattern (mid-ventricular ballooning with sparing of the basal and apical segments) is a variant form.8)9) The dysfunction and regional wall motion abnormalities (RWMA) of the right ventricle (RV) (Fig. 1) are found in 30% of patients who tend to develop congestive heart failure and who have a poor outcome.10)11)
The modified Mayo criteria demand angiographic exclusion of coronary artery disease. In particular, coronary obstructive lesions must be immediately excluded in patients presenting with ST segment elevation. However, a recent report suggested the possible concurrence of coronary artery disease with stress-induced cardiomyopathy.12) Therefore, patients with coronary artery disease should not be excluded for the diagnosis of stress-induced cardiomyopathy if the coronary atherosclerosis is not significant or RWMA extend beyond single coronary artery distribution.
Echocardiographic Characteristics and Hemodynamics
The unique morphology of stress-induced cardiomyopathy is apical ballooning and the relative compensatory hypercontractility of the basal segments. This phenomenon suggests that hemodynamics have an important role. That is, the degree of decreased LV ejection fraction (LVEF) and the existence of left ventricular outflow tract (LVOT) obstruction are the most important parameters in the evaluation and prediction of the severity and prognosis of stress-induced cardiomyopathy.
Initial LV function is usually impaired on hospital admission (mean LVEF, 20-49%) and, in general, resolve within days-to-weeks after initial presentation (mean period, 18 days).3) Most patients achieve a normal LVEF during hospitalization, but a few patients fail to reach the normal range.13) Moreover, a recent study revealed that absence of LV function recovery within 1 week (EF < 50%) was an independent factor associated with mortality.14)
An awareness of LVOT obstruction is an important factor in understanding hemodynamics in stress-induced cardiomyopathy. Basal hypercontractility is one of the characteristics, and can be aggravated with the use of inotropic agents such as dobutamine and dopamine. The Venturi effect around the LVOT results in the movement of the anterior mitral leaflets toward the interventricular septum in the systolic phase ["systolic anterior motion" (SAM)]. The reduction in forward flow contributes to the resultant low cardiac output. This effect may occur in up to one-quarter of patients presenting with a septal bulge associated with SAM and mitral regurgitation (MR).15) Other reports have confirmed structural abnormalities associated with LVOT obstruction, such as mid-ventricular septal thickening (particularly in elderly women).16) LVOT obstruction is a dynamic phenomenon depending on the hemodynamics at that time point, and thus echocardiography is a useful and readily accessible tool if unexplained hypotension or shock is observed. Apical five-chamber and parasternal long-axis views in two-dimensional (2D) images with color Doppler guidance can help in the evaluation of SAM severity. In the parasternal long-axis view, the M mode at the level of the mitral valve may give information about the relationship between the interventricular septum and anterior mitral leaflet.
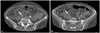
MR can be observed with or without SAM.17)18) SAM can occur concomitantly with MR due to hemodynamic alteration, whereas the mechanism of MR without SAM may be different. The main factor involved in MR without SAM seems to relate to displacement of the papillary muscle, which leads to impaired leaflet coaptation secondary to tethering (Fig. 2). One study showed that patients with significant (moderate-to-severe or severe) acute MR had more depressed LVEF and a less complete and slower recovery of LV function.17) These findings imply that acute MR should be considered to be a potential marker of an adverse clinical course requiring aggressive treatment.
Atypical forms of stress-induced cardiomyopathy have increasingly been reported. Transient mid-ventricular ballooning with preserved basal and apical contractility (inverted takotsubo cardiomyopathy) (Fig. 3) has been described.9)19) The morphology of RWMA can be quite different, varying from a small area of akinesis limited to the LV apex to a large area of LV akinesis.20) Rare (but serious) complications such as LV free wall rupture and consequent death can occur in a manner similar to that seen in patients with MI.21)
Advanced Echocardiographic Techniques
New methods to measure systolic and diastolic dysfunction have recently been developed. Two-dimensional strain is useful to assess and quantify regional and global systolic function. It is based on tracking the movement of stable acoustic patterns ("speckles") within the myocardium frame-by-frame throughout the cardiac cycle.22) Patients with classical stress-induced cardiomyopathy show decreased longitudinal strain values from base to apex. In variant type of stress-induced cardiomyopathy, longitudinal strain is lowest at mid-LV segments. Despite the general perception of basal hypercontractility in stress-induced cardiomyopathy, total longitudinal strain of the LV base is also diminished in several segments at baseline.22)
Recent advances in transthoracic Doppler echocardiography allow non-invasive evaluation of coronary flow velocity and coronary flow reserve (CFR). There is a transient impairment of CFR in the acute phase of stress-induced cardiomyopathy, and this is closely correlated with LV systolic parameters.23)
Contrast echocardiography allows improved visual detection of the endocardial border (particularly the apical area). It is quite useful to use contrast echocardiography to exclude apical thrombi (Fig. 4).24) Contrast echocardiography can also demonstrate abnormalities in myocardial perfusion, which are indicative of microvascular dysfunction.25) Furthermore, normal myocardial perfusion pattern in the akinetic apex helps to discriminate stress-induced cardiomyopathy from anterior wall MI.
Low-dose dobutamine stress echocardiography (DSE) may be a useful and safe tool for the early prediction of myocardial viability in suspected stress-induced cardiomyopathy.26) However, high-dose DSE should be avoided because of the increased risk of induction of stress-induced cardiomyopathy.
Real-time three-dimensional (3D) imaging techniques allow nearly online quantification of the volume and mass of the left ventricle. In particular, rapid image acquisition is possible even in the absence of respiratory and electrocardiographic gating.27) If there are limitations in evaluation with transthoracic echocardiography due to poor windows, transesophageal echocardiography can provide clearer image quality. The relationship between MR and anatomic abnormalities of valves can be clearly observed. The hemodynamics of the LVOT can be easily understood with transesophageal echocardiography. Table 1 and 2 summarize the role of echocardiography in stress-induced cardiomyopathy.
Stratification and Management
There is no established consensus on how to manage stress-induced cardiomyopathy, but early detection of complications can protect against a poor outcome. In most cases, no specific therapy is required due to a favorable prognosis. If needed, diuretics are used to improve pulmonary edema. Although earlier reports suggested the usefulness of beta blocker in this patient population,7)28) a large scale registry data recently published could not find the protective effect of the simple beta blocking agent in preventing the occurrence or recurrence of stress-induced cardiomyopathy.13) Combined alpha- and beta-blocking agent may be advantageous, but this issue should be evaluated in the future.
RV involvement in stress-induced cardiomyopathy is relatively common and RV dysfunction is associated with lower LVEF, longer hospitalizations and more complications such as severe congestive heart failure, intra-aortic balloon pump, and cardiopulmonary resuscitation.10) In addition, Haghi et al.11) reported that pleural effusion was more common in patients with RV involvement and was predictive of RV dysfunction.
LV thrombus is a noteworthy complication and can occur both at initial presentation or at anytime later during the disease course.29) The intraventricular thrombus can be found not only in LV but also RV and left atrial appendage.13)30) The incidence of thrombus formation approximately results in about 2.5% of all the patients with documented stress-induced cardiomyopathy.31) An LV apical thrombus carries a great risk of cerebrovascular accident and distal embolization during the recovery phase of the LVEF (Fig. 5). Anticoagulants and heparin should be given on a short-term basis to patients with decreased LVEF, and short-term echocardiography follow-up is needed to evaluate other complications. Patients with SAM or LVOT obstruction should not be exposed to inotropic agents even if there are in shock.4)
Conclusion
Stress-induced cardiomyopathy is a syndrome with a wide spectrum of hemodynamics and variable prognoses. Echocardiography has many merits thanks to its non-invasiveness, portability, real-time accessibility, reproducibility and concurrent monitoring of anatomic and physiologic abnormalities using conventional (2D and Doppler imaging) as well as advanced diagnostic techniques (strain, tissue Doppler, contrast echo and 3D imaging). Repeat assessment is necessary to monitor recovery or possible complications, and to plan further treatment.





 XML Download
XML Download