

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
While valvular injuries following blunt chest trauma are known to be very rare complication, severe tricuspid regurgitation caused by tricuspid valve injury is the most common cardiac complication following blunt chest trauma.1) The diagnosis of traumatic tricuspid regurgitation may be delayed or missed2-4) because traumatic tricuspid regurgitation is rare complication and traffic accidents have coexisting urgent issues. But it has been reported with increasing frequency, which may be due to the increase in the number of high speed automobile accidents and advances in echocardiography.5)
In most reported cases, traumatic tricuspid regurgitation was frequently missed in emergency department. Although optimal operation timing is important, it is not uncommon to be diagnosed with tricuspid valve injury after several months to years.1-3)6) Here, we report a case of successful repair of tricuspid valve after early detection of severe traumatic regurgitation following blunt chest trauma.
Case
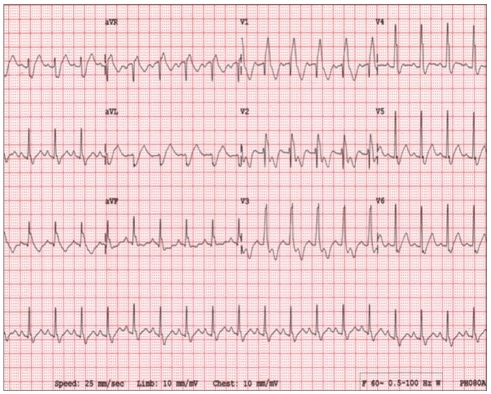
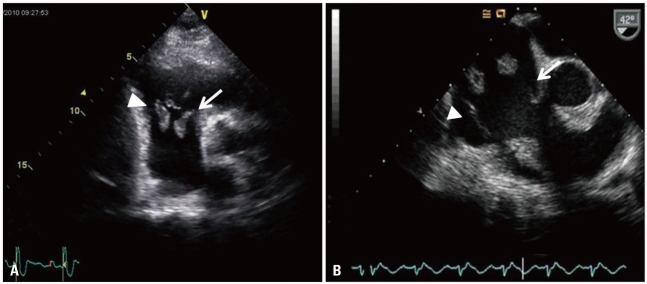
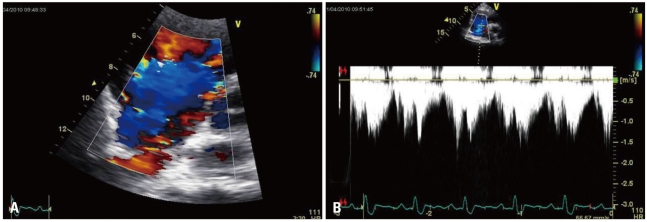
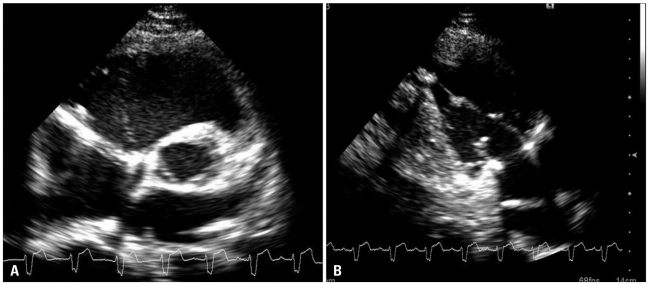
A 19-year-old man, with no past and familial history of heart disease, was brought to the emergency department following a motorcycle accident in which his chest hit the steering wheel with considerable force. He presented left knee, chest and abdominal pain. The patient's vital signs were temperature 36.5℃, heart rate 105 beats per minute, respiration rate 20 per min, blood pressure 100/60 mmHg, and pulse oximetry 98% on room air. On the initial physical examination, a pansystolic murmur was heard along the lower left sternal border with inspiratory accentuation, but signs of right heart failure were not detected. Chest radiograph was normal. Electrocardiogram showed complete right bundle branch block with left posterior fascicular block (Fig. 1). Results of laboratory tests were notable for elevated cardiac biomarker, creatine kinase myocardial band isoenzyme was 144.1 ng/mL, troponin I was 13.88 ng/mL. Echocardiography was performed for evaluation of chest pain and elevated cardiac biomarker. A flail of the septal and anterior tricuspid leaflet was present and rupture of the papillary muscle was suspected on transthoracic echocardiography (Fig. 2A). Although all cardiac structures were identified on transthoracic echocardiography, we performed transesophageal echocardiography to delineate exact anatomy of subvalvular structure. It confirmed prolapse of the septal and anterior tricuspid valve leaflet with large portions of the valve and the subvalvular apparatus protruding into the right atrium indicating rupture of both anterior and posterior papillary muscles (Fig. 2B). Color-flow Doppler echocardiography shows severe tricuspid valve regurgitation (Fig. 3A). Peak velocity of tricuspid valve was 1.62 m/sec and estimated right ventricular systolic pressure was 20.5 mmHg (Fig. 3B). We decided to repair tricuspid valve and referred to thoracic surgery department. Intraoperative findings confirmed the echocardiographic diagnosis of papillary muscle rupture. Tricuspid valve repair was performed with reimplantation of the ruptured papillary muscle and a ring annuloplasty. Postoperative echocardiography showed satisfactory leaflet coaptation (Fig. 4A) and repaired papillary muscle (Fig. 4B). Only mild tricuspid regurgitation remained. The patient discharged from hospital and continues to be asymptomatic after 1 month.
Discussion
The incidence of blunt chest wall trauma and reported traumatic tricuspid regurgitation has been increasing during the last decade.5) However, the diagnosis is difficult because this pathology slowly progress and its presentation can be atypical or asymptomatic, so its incidence rates may be underestimated.2)5)6)
The most common mechanism of acute or subacute tricuspid regurgitation is an anteroposterior compression of the chest with a sudden increase in the right ventricular pressure during the end diastolic phase, when the main pulmonary vessels are compressed. This generates a marked traction on both valvular and subvalvular apparatus.5-8) The usual lesion observed at surgery is subvalvular rupture of the anterior papillary muscle.9) Alternatively, delayed tricuspid regurgitation may be due to papillary muscle contusion with hemorrhage, inflammation, and late necrosis, leading to disruption over time.10) The timing of surgical intervention after traumatic tricuspid regurgitation is a subject of debate. The traditional indication for operation is symptomatic heart failure. But, severe tricuspid regurgitation can result in right ventricular myocardial dysfunction and ventricular dilatation so that operation should be performed before development of myocardial dysfunction and symptom onset.11-13) Another factor to be considered in the optimal operation timing is contusion induced pulmonary hypertension in the acute event. In the treatment of tricuspid regurgitation with contusion induced pulmonary hypertension, postponing surgery to resolve pulmonary hypertension provides successful and durable repair.10) If valve is intact, tricuspid regurgitation is effectively correctable with reparative techniques in an early operation. Also it prevents right ventricular dysfunction.1)3)11)14)
Although there is no current consensus regarding the use of echocardiography as a screening tool, echocardiography is the initial method of choice and it should be performed in all patients with chest trauma, in particular if cardiac injury is suspected, because earlier diagnosis and surgical treatment may increase the feasibility of tricuspid valve repair and prevent progressive deterioration of right ventricular function.1-3)5)12) In some cases, delayed tricuspid regurgitation after blunt chest trauma was reported.7)10) So, if patient has late presentation of clinical signs and symptoms, physicians should consider repeated imaging. Transthoracic echocardiography is often difficult to be performed in some patients with blunt chest trauma because of coexisting chest injuries. In that case, transesophageal echocardiography can safely provide more information of cardiac anatomy involved in traumatic tricuspid regurgitation.7)10) So physicians should consider transesophageal echocardiography if transthoracic echocardiography is inconclusive or cardiac injury is strongly suspicious. In our case, transthoracic echocardiography was enough to know injured tricuspid valvular anatomy, but we performed transesophageal echocardiography to get more information.
This case highlights that physicians should be aware of cardiac complications following blunt chest trauma and using echocardiography as initial examination tools. Although many patients tolerate well many years after the onset of traumatic tricuspid regurgitation, the earlier diagnosis and surgical intervention provide not only prevention of right ventricular deterioration but also feasibility of tricuspid valve repair.
We report a case in which echocardiography was performed as initial screening tool for a young patient presented with chest and abdominal pain after blunt chest trauma, so we could diagnose traumatic tricuspid regurgitation early after admission and performed valve repair operation successfully before right ventricular deterioration.
 XML Download
XML Download