

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pectus excavatum, the most common congenital anomaly of the chest wall, is a malformation of the anterior chest wall characterized by posterior displacement of the inferior part of the sternum with associated prominence of the costochondral junction. This concave chest deformity may displace the heart and squeeze its chambers, especially the right atrium and ventricle.1) In this report, we present a patient with right ventricular (RV) dysfunction caused by pectus excavatum.
Case
A 68-year-old man was admitted to the hospital with New York Heart Association (NYHA) class II exertional dyspnea that has been present for many years. He had no remarkable prior medical history and no history of cigarette smoking or alcohol drinking. His blood pressure was 120/80 mmHg, the pulse rate was 62 beats per minute, and the respiratory rate was 20 beats per minute at presentation. The physical examination did not reveal any abnormal findings except for depression of the chest wall (Fig. 1).
Results of initial laboratory tests, including cardiac enzyme marker levels and thyroid hormone function, were within normal limits. However, B-type natriuretic peptide level was elevated at 314.11 pg/mL.
Initial electrocardiography showed atrial fibrillation without ST-segment elevation or depression or T-wave inversion. Chest X-ray revealed cardiomegaly (Fig. 2).
Transthoracic echocardiography demonstrated a moderately enlarged left atrium, a markedly dilated right atrium, and a moderately enlarged RV with dysfunction. RV ejection fraction by Simpson's rule was 37%. Left ventricular size and function was within normal limits. Stroke volume was 62 mL. A modified 4-chamber view showed a round-shaped RV apex, which was not well visualized in the standard apical 4-chamber view (Fig. 3). The color Doppler image showed the mild tricuspid regurgitation. The peak velocity of the tricuspid regurgitant jet was measured at 2.4 m/s. Tissue Doppler systolic velocity at the tricuspid annulus was 8.0 cm/s (Fig. 4).
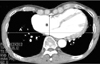
Chest computed tomography with enhancement, which was used to evaluate the precise cause of RV dysfunction, revealed no pulmonary thromboembolism. The RV was compressed by the anterior chest wall. Haller index was determined as 4.2 (Fig. 5). Cardiac magnetic resonance imaging was then obtained to exclude arrhythmogenic RV dysplasia and it failed to show high RV signal intensities, dilatation or myocardial thinning on a T1-weighted image.
We concluded that RV dysfunction in this patient was caused by pectus excavatum. He was treated with an angiotensin converting enzyme inhibitor, coumadin, aspirin, a beta-blocker, and he is followed up regularly at the outpatient department.
Discussion
Pectus excavatum is present in nearly 1 out of every 400 births, and it is more common in male and Down syndrome patients.1-4) Although the etiology of pectus excavatum remains uncertain, overgrowth of the ribs and costal cartilage and defects of the diaphragm have been suggested.4)5) This anatomic alteration produces a reduction in cardiac output and stroke volume and limited lung expansion.6) Therefore, pectus excavatum can induce subjective symptoms of easy fatigability, shortness of breath with exercise or chest discomfort.7)
In a previous report, this chest wall deformity was associated with alteration in RV morphology and function. The reason of RV dysfunction caused by pectus excavatum may be explained by the compression of the heart between the vertebral column and the depressed sternum. Right ventricle is less concentric, more anterior position, and more distensible than the left ventricle. Therefore, this chest wall deformity can produce the global RV dysfunction, irrespective of rounded apex.
Furthermore, suggestive findings of RV dysplasia, such as a rounded RV apex, sacculations of the RV free wall, and hypertrophy of the moderate band, were more common in patients with pectus excavatum.8)
The severity of pectus excavatum can be calculated by the Haller index that is derived from dividing the transverse diameter of the chest by the anteroposterior diameter as measured by computed tomography scanning or chest radiography. The Haller index significantly correlates with RV quantitative measurements, such as RV end-diastolic and end-systolic areas. Normal values of the Haller index are less than 2.5.9) In this case, the Haller index of the patient was 4.2 which is consistent with a severe stage of disease.4)
RV dysfunction is caused by many etiologies such as chronic left heart failure, pulmonary hypertension, valvular heart disease, congenital heart disease.10)11) In the present case, several etiologies for RV dysfunction could be excluded from left heart failure, pulmonary embolism, or, congenital heart disease such as Ebstein's anomaly, hyperthyroidism, and arrhythmogenic RV dysplasia.
Pectus excavatum is a rare cause of RV dysfunction. However, it needs to be suspected in all patents with RV dysfunction. Morphological deformation such as a round-shaped RV apex is especially helpful to differentiate from other causes in patients with RV dysfunction.




 XML Download
XML Download