

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Right atrial aneurysm is a rare disease such that fewer than 60 cases have been reported worldwide.1) In South Korea, only three pediatric cases and no adult cases have been reported.2)3) Right atrial aneurysm predominantly results from a congenital extension of the right atrium; however, its cause has not yet been clarified. In about half of the reported cases, an abnormal finding on thoracic radiography was found incidentally while patients were asymptomatic. These cases can be diagnosed by echocardiography, CT and MRI. If no treatment is carried out, the risk of complications such as arrhythmia and thromboembolism will increase; therefore, medical or surgical treatment is recommended. The following describes the case report of an asymptomatic patient diagnosed with right atrial aneurysm at 69 years of age by echocardiography and CT angiography.
Case
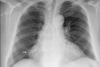
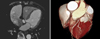
A 69-year-old normally healthy female visited a neighborhood hospital because of intermittent shoulder pain that had started several months earlier, and an abnormality was detected incidentally via thoracic radiography. She was asked to visit a larger hospital and ended up at our hospital. In terms of past history, she had been diagnosed with hypertension three years before and has since been taking antihypertensive medication. Further, her family history showed no specific findings. When she visited our hospital, her blood pressure was 130/70 mmHg, her pulse rate 75 beats per minute, and her body temperature 36.5℃. An electrocardiogram showed 80 beats of normal sinus rhythm (Fig. 1); supraventricular arrhythmia was not found during 24-hour Holter monitoring, and no specific finding was found. However, a thoracic X-ray taken when the patient visited the hospital showed an outstanding heart shadow on the right lower cardiac border, but no abnormality finding was found in the lung parenchyma (Fig. 2). We performed transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) to evaluate the etiology of cardiomegaly. The size of the left atrium and of both ventricles of the heart were normal on the TTE, and the left ventricular ejection fraction (LVEF) was 72%. No abnormality was found in the structure and function of the valves, and abnormal wall motion was not observed. The TTE showed a cystic mass in the right atrial appendage without ultrasonic imaging. The mass was found to suppress the right ventricle during the diastolic phase (Fig. 3A); however, there was no significant limitation of blood flow to the right ventricle during the diastole phase. The TEE clearly showed the shape of the mass connected to the right atrium, which enabled the confirmed diagnosis of right atrial aneurysm (Fig. 3B). The TEE detected a spontaneous echo contrast inside the aneurysm, but no thrombus was found (Fig. 3C). On the CT angiogram, a 9.0 cm×5.2 cm×5.0 cm mass was found in the right atrial appendage, but stricture of the coronary arteries was not found (Fig. 4). The patient was asked to undergo right atrial aneurysm resection, but she denied the procedure and instead started anticoagulant therapy. The progress of her ambulatory care had been being followed up.
Discussion
Since the first report of right atrial aneurysm by Bailey in 1955,4) 60 cases have been reported worldwide. In South Korea, there have been three pediatric cases of right atrial aneurysm, with no adult case ever having been reported. The patients ranged in age from 32 weeks' gestation to 75 years at the time of diagnosis. Forty-eight percent of the reported patients had no symptoms, and other patients complained of arrhythmia, palpitations, shortness of breath, and fatigue. Normal sinus rhythm was observed on the electrocardiograms for 53% of the patients, and atrial fibrillation and flutter was observed in about 28%. In some cases, pre-excitation syndrome, junctional rhythm, heart block, supraventricular tachycardia, and so forth were reported,1) but the correlation between atrial aneurysm and arrhythmia has not yet been clarified. Most cases of asymptomatic right atrial aneurysm are discovered by chance as cardiomegaly with thoracic radiography. These cases can be easily diagnosed non-invasively by TTE, CT angiography, and so forth. If the result of diagnosis by the above methods is uncertain, TEE or cardiac MRI may be conducted. In this case, right atrial aneurysm was diagnosed by echocardiography, and CT angiography provided a certain diagnosis. Cardiac MRI was not performed because CT angiography is its equivalent in clarifying the structure of the coronary arteries, in relation to surrounding structures through three-dimensional reconstruction.5) Patients with right atrial aneurysm are known to have a high risk of supraventricular arrhythmia, stroke, and thromboembolisms including pulmonary thromboembolism; these risks have also been reported for left atrial aneurysm.6) Chatrath et al.4) reported that right atrial aneurysm might cause an extended tricuspid annulus due to an extended right atrium as well as tricuspid regurgitation. Therefore, anticoagulant therapy should be started upon diagnosis of right atrial aneurysm in order to prevent such complications. Ultimately, right atrial aneurysm resection should be performed. Since Morrow and Behrendt carried out the first right atrial aneurysm resection in 1968,7) surgical treatment has been reported several times to date. When cardiomegaly is found by chance on the thoracic radiogram of an asymptomatic patient, Ebstein's anomaly, pericardial effusion, pericardial cyst, tumor and so forth must be eliminated as possible causes.8) Whether to perform surgical treatment, for example, right atrial aneurysm resection, or to proceed non-surgically with continuous anticoagulant therapy in a patient with asymptomatic right atrial aneurysm is still considered controversial. However, surgical treatment should be preferentially recommended due to the possible risk of death owing to complications of arrhythmia and thromboembolism.9)10) This particular case is extremely rare, as it is the first instance of right atrial aneurysm found incidentally in old age in South Korea. Even though specific clinical symptoms and arrhythmia were not found, we recommended surgical treatment due to the risk of death from complications. However, she denied the treatment for the reasons of old age and a lack of symptoms. Currently, her progress is being observed with medication.


 XML Download
XML Download