

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Coronary arteriovenous (AV) fistula is referred to as an abnormal communication between one of coronary arteries and a cardiac chamber or a great artery or the vena cava. It is a rare congenital abnormality and usually asymptomatic at a younger age.1) However, two thirds of patients more than 20 years of age have symptoms of congestive heart failure, pulmonary hypertension or uncommonly angina pectoris.2)3) Although recent advance in cardiac imaging modalities including cardiovascular computed tomography (CT) or magnetic resonance imaging provide us a unique opportunity to accurately detect and confirm congenital coronary abnormalities noninvasively, transthoracic echocardiography (TTE) is widely used as a first screening tool thanks to its versatility as well as relative advantages over the other modalities in terms of expense and radiation.4)5) Aside from straightforward evaluation of cardiac anatomy and function, we can sometimes catch the clues to the presence of enlarged coronary arteries or abnormal Doppler color flow originated from or drained into abnormal sites.6) We here describe right coronary artery-to-main pulmonary trunk fistula without aneurismal change in an asymptomatic patient, which was initially suspected on routine TTE examination.
Case
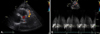
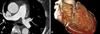
A 71-year-old woman was referred to the nephrology outpatient clinic to establish long-term treatment plans for chronic kidney disease (CKD). She had a previous history of diabetes mellitus and hypertension and had taken anti-diabetic and anti-hypertensive medications. After she slipped down 3 days earlier, she was admitted to local clinic and was diagnosed as having rib fractures and renal dysfunction. The patient complained of no symptoms except leftsided chest pain on coughing. During physical examination, she was alert and well-oriented. Her blood pressure was high (158/82 mmHg) and heart rate was 82 beats/min. The chest was clear on auscultation and no abnormal murmur was heard. The electrocardiogram showed normal sinus rhythm and the chest X-ray displayed neither sign of pulmonary congestion nor cardiomegaly. TTE showed a mildly dilated left ventricle (LV) with low borderline LV systolic function (EF = 50%) and normal LV wall thickness. On the parasternal short axis view at the level of aortic valve, an abnormal Doppler color flow was found near the main pulmonary trunk, which seemed to take a course toward the echocardiographic probe (Fig. 1A). Pulsed wave Doppler echocardiography showed a continuous flow throughout the cardiac cycle with a predominant flow in diastole, suggestive of coronary artery blood flow (Fig. 1B). To confirm the presence of congenital coronary AV fistula, CT coronary angiography was performed. As a result, a conal branch of right coronary artery-to-main pulmonary trunk fistula with multiple channels like a ground cherry was found (Fig. 2). Controversial debate exists with regard to whether to treat or not patients with coronary AV fistula incidentally detected. Given that she was totally asymptomatic and it was small in size with no aneurismal dilation, we decided not to perform elective ligation. After artificial AV fistula formation for hemodialysis was conducted, she has been uneventfully followed at the outpatient clinic without any cardiovascular symptom.
Discussion
Congenital coronary anomalies consist of anomalous origin and course of coronary artery, anomalies of intrinsic coronary arterial anatomy and congenital coronary AV fistula. Congenital coronary AV fistula was first described by Krause7) in 1865, and it is found in 0.1-0.8% of patients who undergo coronary angiography.8-10) It is commonly originated from the right coronary artery in 55%, the left coronary artery in 35% and both in 5%,11) whereas most of coronary AV fistula is terminated in the right side of the heart; i.e. right ventricle in 41%, right atrium in 26%, and pulmonary arteries in 17%.12) A fistula draining the blood flow from the conal branch of the right coronary artery to the pulmonary trunk, as in our case, is an unusual form of coronary AV fistula.13)
Patient with coronary AV fistula are generally asymptomatic in the first two decades. As patients are getting older, the frequency of both symptoms and related complications increases.14) Common symptoms include chronic fatigue, exertional dyspnea, angina or myocardial infarction, all of which can be explained by 'coronary steal' phenomenon. In general, asymptomatic coronary AV fistula is commonly diagnosed due to cardiac murmur and thus patients with coronary AV fistula in whom cardiac murmur is not audible remain undetected. Although timely identification of anomalous origin of coronary arteries is known to be of paramount importance given its contribution to sudden, unexpected cardiac deaths in young subjects,15) implication of early recognition of congenital coronary AV fistula is unclear.
In this case, a 71-year-old woman had no symptoms suggestive of left-to-right shunt or myocardial ischemia. On physical examination, cardiac murmur was not heard and there was no clinical clue suspicious of the presence of coronary AV fistula. The only hint indicative of its presence was abnormal Doppler flow close to the main pulmonary trunk that was fortuitously detected on TTE. Albeit the opposite direction of color Doppler flow in comparison with the usual shunt direction, i.e. away from vs. toward the main pulmonary trunk, congenital coronary AV fistula was highly suspected. Thus, noninvasive CT coronary angiography was performed for confirmation and revealed a conal branch of the right coronary artery-to-main pulmonary trunk fistula. Aneurismal dilatation was not observed and proximal part of right coronary artery was not dilated, either. Because coronary AV fistula usually contains conglomerated vessels as in our case, the direction of color Doppler flow could be opposite to shunt direction depending on the position and angle of the probe. Based on this fact, every effort had been made to detect the color Doppler flow toward the main pulmonary trunk, but we could not find any flow draining into the pulmonary trunk. Therefore, the fact that direction of Doppler color flow is away from the main pulmonary trunk cannot exclude the possibility of the presence of congenital coronary AV fistula. On the contrary, detection of abnormal Doppler flow during diastole regardless of flow direction should be followed by suspicion of the presence of coronary AV fistula.
Despite many reports till now, management of coronary AV fistula patients has still not been clearly defined. Generally, symptomatic coronary AV fistula is managed with surgical ligation or occlusion by interventional catheterization.16)17) Antiplatelet therapy, such as low-dose aspirin, is recommended and prophylactic precautions for subacute bacterial endocarditis are also recommended.8) If the patient is asymptomatic, measurement of shunt ratio (Qp/Qs) by cardiac catheterization has clinical importance especially in children because frequency of symptoms increases as patients are getting older.14) However data are lacking concerning the treatment of incidentally-found and asymptomatic coronary AV fistula in adults. Therefore, decision to perform surgical ligation or interventional occlusion should be made case-by-case. We believe that asymptomatic, old patient without aneurismal dilation of the coronary artery can be safely managed without surgical or interventional treatment, as in our case.
In conclusion, we report here a rare case showing a conal branch of the right coronary artery-to-main pulmonary trunk fistula detected by chance on TTE in an asymptomatic, old patient.
 XML Download
XML Download