

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Lipoma in the heart is very rare. Although most cases don't cause symptoms, some of them are symptomatic according to their location and size. We report a patient with a large lipoma in right atrium, who suffered from intermittent angina and have been relieved from the symptom after surgical removal of the tumor.
Case
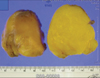
A 54-year-old woman visited the emergency department due to chest pain for 3 hours associated with diaphoresis. She had suffered from symptoms of angina, which were triggered sometimes, not always, by positional change like standing from squatting, rotating the chest, walking or jogging. Her electrocardiogram was normal. Her cardiac enzymes were within normal ranges. Exercise electrocardiogram revealed no abnormal finding. Transthoracic echocardiography demonstrated a mass (about 3×4.5 cm diameter) arising from the free wall of right atrium, and sparing tricuspid valve (Fig. 1A). We believed it was a well-capsulated primary cardiac tumor, such as a myxoma or lipoma. Chest computed tomographic scan showed a well-capsulated cardiac tumor that had same density with subcutaneous fat, suggesting lipoma rather than myxoma (Fig. 2). Transesophageal echocardiography also revealed a mass arising from the free wall, sparing tricuspid valve (Fig. 1B). We performed coronary angiography to exclude coronary artery disease, which showed no significant stenosis (Fig. 3A). Right atriogram showed a round well-demarcated, redundant mass in the right atrium (Fig. 3B). We thought the tumor might compress the right coronary artery, resulting in intermittent typical angina although it was not seen on conventional coronary angiography. She was referred to surgery. An 5×6 cm encapsulated mass with broad base from the right atrial free wall was found, and excised without any tricuspid leaflet. The histopathology demonstrated that the yellow well-capsulated mass was consistent with lipoma (Fig. 4). The postoperative course was uneventful. The patient was discharged on postoperative day 7. Until now after the surgical removal of the right atrial lipoma, she has not suffered from any angina for 6 months yet.
Discussion
Cardiac lipomas account for 4% to 10% of benign cardiac tumors.1)2) They are well-encapsulated tumors typically composed of mature fat cells. True cardiac lipomas are much less frequent than lipomatous hypertrophy of the interatrial septum, but they can occur in almost any location of the heart. Symptoms are not characteristic and depend on the lipoma's location and size.4) Most cases are asymptomatic. However, they can cause arrhythmias, embolize, compress the coronary arteries, or obstruct flow within the heart.3) Surgical removal of the tumor is warranted in symptomatic patients, while surgical treatment of asymptomatic patients is not always called for.5) In the present case, the patient sometimes has suffered from angina, and her coronary angiogram revealed no significant stenosis. So we thought the tumor might compress the right coronary artery, resulting in intermittent typical angina. After successful surgical excision of the tumor, she has not suffered from angina for 6 months.



 XML Download
XML Download