

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Rupture of sinus of Valsalva is a fatal disease requiring surgical management.1-3) A spontaneous rupture of sinus of Valsalva associated with congenital and acquired aneurysm has been infrequently reported.4)5) Also, an iatrogenic dissection and rupture of the aortic sinus of Valsalva during catheterizations of the related coronary artery is rarely reported.6)7) But, a spontaneous perforation of sinus of Valsalva without structural anomaly and iatrogenic trauma has not been reported in our best knowledge. This patient was presenting with transient ST elevation in inferior leads due to compressing the right coronary artery (RCA) by hematoma attributed to spontaneous perforation of sinus of Valsalva. Surgical repair was successfully done. There was not any associated disease in the sinus of Valsalva, aortic valve or coronary arteries.
Case
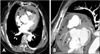
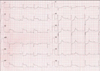
A 66-year-old female was admitted to our cardiovascular center. She suffered from recurrent, brief substernal pain at resting state from 24 hours ago. She had the history of hypertension for 3 years. But, she had no other risk factors of coronary artery disease such as diabetes mellitus, hypercholesterolemia, smoking and family history. On admission, her blood pressure was 120/80 mmHg and her heart rate was 80 bpm. No other abnormalities were found on physical examination. The troponin I was not elevated. The chest X-ray showed mild cardiomegaly and mediastinal widening (not shown). The initial electrocardiogram showed non-specific ST-T change (not shown). At first, routine computed tomography (CT) was done for the exclusion of aortic dissection or aortic pathology. Routine CT showed large hematoma adjacent to the RCA, therefore we thought focal dissection, coronary artery rupture or rupture of sinus of Valsalva at that time. (Fig. 1A). The transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) showed a significant amount of pericardial effusion and hyperechogenic mass-like lesion adjacent to the junction between right ventricle (RV) wall and right atrium (RA) wall (Fig. 2). But, we didn't find any aortic pathology. The coronary angiography (CAG) was performed safely and showed normal coronary arteries without any significant stenosis and rupture (Fig. 3). At one hour after CAG, the chest pain recurred accompanying with cold sweating. Her blood pressure decreased to 80/60 mmHg, and ECG showed ST elevation at II, III, aVF and ST depression of V4-6 with complete atrioventricular block (Fig. 4). However, the symptoms and ECG abnormality were spontaneously subsided. The rechecked 64-channel Coronary Multidetector CT (MDCT) showed increased size of hematoma and the extravasation site from the junction between right and noncoronary sinus of Valsalva (Fig. 1B).
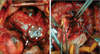
Surgical primary repair was performed immediately. We found 0.5 cm sized transverse tearing in sinus of Valsalva at just above commissure between noncoronary cusp and right coronary cusp (Fig. 5). The large hematoma from the perforation site was compressing proximal RCA and bursting into the RV, RA and pericardial space (Fig. 5). There was not any associated disease in the sinus of Valsalva, aortic valve or coronary arteries except a small perforation. The patient's serologic markers for syphilis and other connective tissue disorders such as rheumatoid arthritis and systemic lupus erythematosus were all negative. The patient was stabilized after primary surgical repair and has been asymptomatic during 6 month follow-up.
Discussion
Rupture of Sinus Valsalva is a very rare, life-threatening cardiovascular event.1-3) This is usually associated with congenital and acquired aneurysm. Acquired aneurysm was developed by conditions such as cystic medial necrosis, syphilis, Marfan's syndrome, subacute bacterial endocarditis, ankylosing spondylitis and rheumatoid arthritis.8-12) An enlarging unruptured aneurysm produces symptoms by compression of an adjacent chamber. The ruptured aneurysms usually presented by cardiac tamponade and acute heart failure due to right to left shunt.1-5) Iatrogenic localized dissection of the sinus of Valsalva also is an extremely rare accident that may occur during percutaneous coronary intervention (PCI). It can lead to serious complications such as rupure of the sinus of Valsalva and dissection of the ascending aorta.6)7) Iatrogenic coronary artery dissection involving the adjacent aortic wall has been treated successfully with conservative treatment, sometimes stenting and surgery.6)7) In our case, rupture of the sinus of Valsalva was not accompanied with other associated pathologies such as aneurysm and trauma.
An important question is why ischemic symptom compressed by hematoma subsided spontaneously. First, we hypothesize that this hematoma might be not mature at that time. It may be a mixed form of transient blood collection and real hematoma in a limited space which might be compressing the RCA when bleeding was active. If bleeding was stopped, the compressing effect would be relieved because temporarily collected blood might spread into adjacent tissue space from the limited space. The 64 channel MDCT was able to demonstrate active bleeding from sinus of Valsalva. Second explainable hypothesis is the ischemic symptom may be associated with coronary artery spasm due to close contact of hematoma to the artery.
Unfortunately the size of hematoma and the amount of pericardial effusion were increased after diagnostic CAG. Whether diagnostic CAG may facilitate the bleeding is unknown. In this case, the diagnostic CAG might not have been necessary because 64-channel MDCT was enough to evaluate coronary arteries. The diagnostic CAG should have been considered more carefully if any bleeding is suspicious.
This presenting case showed spontaneous perforation of Sinus of Valsalva without the associated aortic wall pathology such as aneurysm could occur, although extremely rare. Furthermore, active bleeding from sinus of Valsalva may induce not only persistent ischemia but also transient ischemia by compressing to coronary artery.


 XML Download
XML Download