

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Causes of cardiac mass are so various. Thrombus, primary tumor, metastasis, and vegetation can make a mass in various site of heart. Recently, many cardiac masses have been detected by the advanced image modality, such as echocardiography and chest computed tomography (CT). We present the case of simultaneous two cardiac masses with different etiologies.
Case
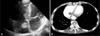
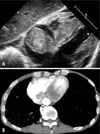
A 76-year-old male was referred for cardiac masses on chest CT which was performed to evaluate adenocarcinoma of lung. He was already found metastasis to adrenal gland. He underwent a transthoracic echocardiogram, which revealed two cardiac masses. One was located in interventricular septum of base level, and the other was oscillating in right atrium (Fig. 1 and 2). It seemed that they contacted with each other via tricuspid annulus. No vascular flow at inside of mass was found. Transthoracic echocardiography showed neither valvular dysfunction or left ventricular systolic dysfunction. Low extremity doppler ultrasound showed no evidence of deep vein thrombus. Though electrocardigram (ECG) shows T wave inversion in inferior leads, ECG monitoring during admission (14 days) revealed no specific arrhythmia like ventricular tachycardia. In pulmonary artery CT angiogram showed no evidence of pulmonary embolism. Mass at interventricular septum was not located in ventricular cavity and was involved intramyocardium, which implicated that it might be tumor rather than thrombus. In the other hand, the mass in right atrium oscillated in atrial cavity. So we interpreted two masses as metastasis and thrombus respectively, and then started chemotherapy for lung cancer and low-molecular heparin for thrombus. However, he was diagnosed as pulmonary tuberculosis 4 weeks later. He had a hemoptysis and the treatment for cancer and thrombus should be interrupted. After seven weeks follow up, the size of two cardiac masses were increased (Fig. 3). Interventricular septal metastasis was from 3.7 cm × 2.4 cm to 4.8 cm × 3.1 cm, and right atrial thrombus was from 1.7 cm × 1.5 cm to 3.6 cm × 3.3 cm. His poor performance and advanced age make it difficult to carry out further chemotherapy, and he was expired during supportive care.
Discussion
Myocardial metastasis has been known to be a rare condition. However we have been confronting undetermined myocardial lesions in autopsy case or in clinical practice because of prolonged survival of cancer patients and better diagnostic tool.1-3) For their similar characteristics and morphologies in chest CT and echocardiography, distinguishing metastasis from thrombus is intricate task, but it is critical for treatment plan and outcome. Also patients with malignancies have hypercoagulable tendencies that are predisposed to develop thrombus easily. Metastasis, especially in ventricle, may result in dangerous arrhythmia or ventricular outflow disturbance, and thrombus may cause fatal subsequent outcomes such as pulmonary embolism. Clinically differential diagnosis of these lesions is more complicated, because invasive diagnostic procedure like myocardial biopsy is rarely available in advanced cancer patients like our subject. Therefore diagnosis almost depends on clinical finding like location, morphology, and response for treatment. Atrial involvement can be evaluated and diagnosed easily than ventricular lesion because it usually invades the myocardium directly from vena cava or pulmonary structure in metastasis and thin atrial myocardium help us to differentiate metastasis from normal myocardium. But ventricular involvement is far more intricate and no previous reports about differential diagnosis augment this difficulty. Morphologically, metastasis to the myocardium manifested as round and compact shape, it usually have a well demarcated border rather than thrombus. Magnetic resonance imaging or transesophageal echocardiography may be helpful sometimes.
In addition, denudation of endocardium by cardiac mass may make it easy to develop thrombus or resultant embolus, so anti-coagulation is needed in most cases. Surgical resection may be considered as treatment option, however, systemic chemotherapy is main trend of management. Though there are several reports about myocardial metastasis or thrombus respectively, we present the case with metastasis and thrombus simultaneously.4)5)

 XML Download
XML Download