

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Evaluating the left ventricular (LV) contractile function in patients with severe mitral regurgitation (MR) is a difficult clinical problem. Because of the favorable loading condition,1) ejection phase indexes such as ejection fraction (EF) may remain in the normal range despite the presence of significant contractile dysfunction and mislead the decisions regarding the indications and timing of surgery.2-7) Among many parameters proposed as a measure of myocardial function,8-17) Doppler-derived rate of LV pressure rise during ventricular contraction (dP/dt-Doppler) has been shown to correlate well with peak dP/dt measured by cardiac catheterization and thus postoperative LV function.18) However, it is limited clinically due to the complexity of the measurements and the difficulty in obtaining appropriate Doppler tracing in patients with eccentric MR.
Doppler tissue imaging (DTI) is a relatively new ultrasound algorithm that records systolic and diastolic velocities within the myocardium. The velocity of annular motion obtained by DTI reflects the rate of LV volume change in the long-axis dimension19-21) and, therefore, LV systolic and diastolic function. Although systolic mitral annular velocity has been shown to reflect peak dP/dt,22) it has not been fully tested in the presence of significant MR in which predominant increase of preload occurs. Therefore, we performed the study to test whether the systolic mitral annular velocity correlates with parameters associated with left ventricular rate of pressure rise.
Methods
Study population
Sixty-two patients who had chronic 3+ or 4+ MR with normal LV EF (>50%) were enrolled. Twenty-five patients were men and 37 patients were women; mean age was 47±15 years (range: 24-77). The etiology of MR was myxomatous degeneration in 55 patients and rheumatic involvement in 7. Patients with coronary artery disease, mitral stenosis, other valvular diseases, pulmonary disease and atrial fibrillation were excluded. All patients were fully informed about the procedure and gave informed consent.
Echocardiographic examination
All patients underwent standard 2-dimensional and Doppler echocardiography. Echocardiographic examinations were performed with commercially available equipment (Siemens Sequoia, Mountain View, California, or Vivid 7, GE Medical System, Horten, Norway).
LV end-diastolic and end-systolic volumes were measured using biplane Simpson method. Peak systolic mitral annulus velocity was measured in apical 4-chamber view using Doppler tissue imaging with the sample volume at the septal annulus. Forward stroke volume was calculated as LV outflow tract area multiplied by the time integral of the outflow tract velocity measured by pulsed-wave Doppler.
Outflow tract area was determined as D2π/4, where D is its diameter measured from a zoomed systolic freeze-frame in the parasternal long-axis view. Total stroke volume was calculated as mitral annulus area multiplied by the time integral of the transmitral flow velocity measured by pulsed-wave Doppler with the sample volume at the mitral annulus level. Mitral annulus area was determined as D1D2π/4, where D1 and D2 are major and minor axis diameters measured from a zoomed early diastolic freeze-frame in apical 4- and 2-chamber view.23)24) Regurgitant stroke volume was calculated from the difference between total and forward stroke volume and regurgitant fraction was calculated as the ratio of regurgitant stroke volume to total stroke volume. Systolic pulmonary artery pressure (PAP) was derived from the tricuspid regurgitant jet velocity with the simplified Bernoulli equation with assuming a right atrial pressure of 10 mmHg.
The rate of systolic LV pressure rise (dP/dt-Doppler) was estimated from a continuous-wave Doppler of MR jet as previously described.25) Briefly, the time for the MR velocity to increase from 1 to 3 m/sec was carefully measured and divided by 32 mmHg that represents the LV pressure rise during this period. All echocardiographic measurements were averaged for three beats for patients in sinus rhythm.
Cardiac catheterization
In 10 patients undergoing mitral valve surgery, left-sided cardiac catheterization was performed through the femoral approach before the operation. The time interval between the echocardiographic examination and cardiac catheterization was <24 hours in all patients. Left ventricular pressure was measured before angiography. An 8F pig-tail catheter was placed in the left ventricle and a 3F micromanometer (Millar Instruments) was introduced into it. Care was taken to avoid premature ventricular contraction. Pressure wave forms were recorded on a Sony digital audio tape recorder with a sampling rate of 600 Hz for later analysis.
The micromanometer system was calibrated electronically after equilibration against the pressure recorded through the fluid-filled catheter. The zero-pressure reference was set at midchest. Peak left ventricular dP/dt was obtained by electronic differentiation of the left ventricular pressure pulse. To exclude respiratory variation, pressures were measured during end-expiratory apnea.
Electrical signals of pressure were digitalized using the standard MATLAB 7.0.4 packet. The first derivatives of pressure rise of LV were obtained and the mean values of 20 consecutive cardiac cycles were used in the analysis.
Statistical analysis
All values are expressed as means ± SD or as percentages. Comparisons of the continuous variables were performed using the unpaired t-test. Pearson's correlation analysis was employed to compare the relationship of Doppler-derived dP/dt, Peak dP/dt-cath, S' velocity and EF. All statistical analyses were performed with SPSS 13.0 (SPSS Inc., Chicago, Illinois), and P values of <0.05 were taken to indicate statistical significance.
Results
Baseline characteristics
Mean LV ejection fraction was 60±6% and regurgitant fraction was 59±15%. Despite normal LV ejection fraction, peak dP/dt-Doppler ranged from 710 to 2133 mmHg/sec with the mean value of 1376±410 mmHg/sec. Table 1 and 2 summarized the baseline clinical and echocardiographic characteristics of 62 patients.
The impossible integration of MR jet due to the eccentricity according to the etiology of MR
It was impossible to integrate MR jet by a continuous-wave Doppler-echocardiography in 32 patients with eccentric jet direction (52%). 53% of 55 patients with degenerative change and 29% of 7 patients with rheumatic involvement had eccentric MR. But no statistical difference between 2 groups did not be shown (p=0.43).
Mitral annulus velocity and parameters reflecting left ventricular contractile function
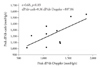
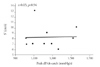
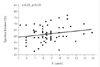
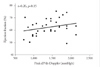
S' velocity correlated well with LV dP/dt-Doppler (r=0.50, p<0.01) (Fig. 1). In 10 patients who underwent LV catheterization, LV dP/dt-Doppler correlated well with peak dP/dt-cath (r=0.68, p=0.03) (Fig. 2). S' velocity could be measured in all patients. However, S' velocity did not correlate with LV dP/dt-cath (r=0.03, p=0.94. Fig. 3) and EF (r=0.21, p=0.10, Fig. 4). Also, EF did not correlate with preoperative LV dP/dt-Doppler statistically (r=0.26, p=0.15) (Fig. 5).
Discussion
It is difficult to assess LV contractile function in patients with MR accurately because of an abnormally decreased afterload, increased preload and altered impedance to LV emptying. Previous studies reported that a significant portion (as much as 47%) of the regurgitant volume could occur before opening of the aortic valve.2)26) So the ejection phase indexes such as EF had the limitation to represent the LV contractility in MR.
The maximum rate of rise of LV systolic pressure, peak dP/dt is one of the oldest and most widely used measures of myocardial contractility. Previous studies showed that peak dP/dt rises with increases in afterload and preload, but the changes were quite small (<10%) in the physiologic range.27) Also, peak dP/dt was known to reflect LV function of isovolumic phase, in which most of regurgitation was developed.28) Therefore, it must be better to represent LV contractility in MR among other parameters. However, the clinical use of peak dP/dt has been limited because accurate measurement conventionally requires an invasive high-fidelity pressure transducer recording during cardiac catheterization.
LV dP/dt by continuous wave Doppler echocardiography has been proposed by GS Bargiggia and his collegues for the noninvasive estimation of peak dP/dt in patients with MR.25) It correlated well with invasive measurement of peak dP/dt. Despite the advantage of the parameter such as noninvasiveness, serial measurement and reproducibility, its clinical application is limited because of the complexity of the measurements and the difficulty in obtaining appropriate Doppler tracing in patients with eccentric MR.
Present study showed that the MR jet was traced in only half of patients. Although no statistical difference between two groups, degenerative MR was more eccentric than rheumatic MR. Mitral valve prolapse and chordal rupture are included in degenerative MR and these etiologies may involve one valve leaflet more likely than rheumatic MR. Therefore, we can explain this difference of proportion of MR jet.
Doppler tissue imaging is a useful noninvasive technique for recording systolic and diastolic velocities within the myocardium. The velocity of annular motion obtained by DTI reflects the rate of LV volume change in the long-axis dimension. It was reported that peak systolic mitral annulus velocity reflected peak dP/dt without significant MR.22) But in changing loading condition such as MR, its role has not been proven.
At first we investigated the feasibility of this parameter. We could obtain S' velocity in all patients. Signal-to-noise ratio and temporal resolution are relatively high in DTI and just visualization of mitral annulus makes S' velocity obtained. Therefore, it was very feasible parameter.
Next, we investigated the relationship between S' velocity and other parameters associated with left ventricular rate of pressure rise. Present study showed that S' velocity correlated well with LV dP/dt-Doppler but EF did not. This result can be interpreted for two reasons. Firstly, because DTI indices are known to be relatively load-independent. No correlation between S' and EF may also result from this load-independency of S'. Secondly, because the activation of myocardial fibers may happen sequentially. Long axis shortening from longitudinal subendocardial fibers occurs before short axis shortening during the isovolumic contraction phase.29) S' velocity represents the change of long axis dimension. So it may reflect LV contractility more sensitively than EF affected by the loading condition. However, the decrease of preload by regurgitation already starts in the isovolumic contraction phase and thus the change of longitudinal dimension may not reflect LV true forward contractiliy. Therefore, further studies about the difference between longitudinal and radial contraction will be necessary.
Moreover, The present study showed the good correlation between S' and peak dP/dt-Doppler, but it was not sufficiently high (r=0.50). Both of S' and peak dP/dt-Doppler represent LV systolic function, however, peak dP/dt-Doppler includes the isovolumic contraction phase and S' represents mainly systolic function in the ejection phase. This time difference of each parameter might show the modest correlation.
The main limitation of this study is the relatively small patient group. Previous studies and our data showed that LV dP/dt-Doppler correlated well with peak dP/dt-cath.22)28) But our data did not show that S' correlated with peak dP/dt-cath. Further studies with larger patient groups should confirm that S' would correlate with peak dP/dt-cath.
Also, the correlation coefficient between dP/dt-Doppler and peak dP/dt was not sufficiently high. However, dP/dt-Doppler was an average slope determined by 2 points on the LV pressure rise and it can underestimate the true peak dP/dt.28) Our data also showed this underestimation.
Conclusion
In conclusion, Systolic mitral annulus velocity is a simple and feasible marker of LV dP/dt and, therefore, may be useful for assessing myocardial contractile function in patients with MR. It may be helpful to find subgroup for mitral surgery and follow up this individuals non-invasively and repetedly. Further studies should also clarify the relationship between S' and postoperative EF or clinical outcomes.



 XML Download
XML Download