

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic cough, defined as a cough lasting more than 8 weeks, is common.1 The most common causes of chronic cough are asthma, gastroesophageal reflux disease, and postnasal drip syndrome,2 and the accuracy of diagnosis is assessed by the response to specific treatment in most cases. Assessing the effectiveness of management is also required for a subgroup of chronic coughers in whom a diagnosis cannot be made even after thorough and systematic investigation.3 Thus, assessment of cough using validated cough severity outcome tools is important in the management of and research into chronic cough. A few tools, including cough specific quality-of-life questionnaires, have been recommended.3 However, there are no specific tools for measurement of chronic cough in the Korean population.
The Leicester Cough Questionnaire (LCQ), a widely used cough-specific quality-of-life questionnaire, has been shown to be repeatable and responsive, and correlates with cough frequency in chronic cough.3,4 This study was conducted to develop a Korean version of the LCQ and determine its reliability, validity, and responsiveness.
Since there are no well validated outcome measures in chronic cough, we could not explore the relationship between the Korean version of the LCQ and other objective markers of cough severity. Thus we evaluated the relationship between the Korean LCQ and subjective measurements of cough severity such as cough visual analogue scale (VAS) and cough symptom score, and the relationship between the Korean LCQ and Short-Form 36 (SF-36) which is a measurement of generic quality of life but not specific for cough. These methods have been used in development and validations in other languages of the LCQ.4,5
MATERIALS AND METHODS
Patients
Patients with chronic cough were enrolled from five university hospitals (Hanyang University Guri Hospital, Samsung Medical Center, Seoul National University Hospital, Seoul National University Bundang Hospital, and Kangwon National University Hospital) between May 2011 and October 2013. Chronic cough was defined as a cough lasting more than 8 weeks. Patients aged <15 or ≥70 years old were excluded. Enrolled patients completed two questionnaires, the LCQ and the SF-36 upon presentation and completed the LCQ and the Global Rating of Change (GRC) upon follow-up visits after 2-4 weeks. Patients were graded using a 100-mm linear VAS of cough severity from "no cough" to "worst cough" and cough symptom score at each visit. The study protocol was approved by the Institutional Review Board of each participating hospital, and informed consent was obtained from all patients.
Leicester Cough Questionnaire
The LCQ is a cough-specific quality-of-life questionnaire containing 19 items divided into 3 domains (physical, psychological, and social). A 7-point Likert scale is used to evaluate the responses for each item, and domain scores range from 1 to 7. Thus the total score is 3-21; a higher score indicates a better quality of life. The LCQ was adapted for Korean conditions following a forward-backward translation procedure, with independent translations and counter-translations. The Korean version was tested in 3 patients with cough for the suitability of wording and phrasing.
Short-Form 36 (SF-36)
SF-36 is a generic quality-of-life questionnaire which is a well-tested and validated generic health status measure. The time scale over which the symptoms or events being questioned in SF-36 was adjusted to 2 weeks to be consistent with the LCQ in this study. SF-36 contains 36 items divided into 8 scales (physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health) and 2 dimensions (physical health and mental health).6 Scores of each LCQ domains (physical, psychological and social) were compared to SF-36 physical health dimension score, SF-36 mental health dimension score, and SF-36 social functioning scale score, respectively.
Other measurements
The cough symptom score is a numeric cough score consisting of two questions regarding subjective cough severity during the day and the evening.7,8 Scores for each question range from 0 to 5, and thus the cough symptom score ranges from 0 (no cough at all) to 10 (maximum cough). The GRC assessment was performed to evaluate self-perceived changes in disease control since the first visit. Responses were scored from +7 (a very great deal better) to -7 (a very great deal worse) and classified as unchanged (-1, 0, +1), small change (-3, -2, +2, +3), moderate change (-5, -4, +5, +4) and large change (-7, -6, +7, +6).9 Scores of +4, +5, +6, and +7 were considered to represent clinically significant improvement.10
Validation
Concurrent validity
Concurrent validity is the assessment of an instrument against other standards; it was assessed by correlating the LCQ scores with SF-36, the cough symptom score, and VAS. A correlation coefficient ≥0.4 is generally regarded as a moderate correlation and >0.75 as a strong correlation.
Internal consistency
Internal reliability of each domain was assessed by determining Cronbach's alpha coefficients, which indicate the extent to which items are related. Internal reliability is generally acceptable if Cronbach's alpha coefficient is greater than 0.7.
Test-retest reliability
The repeatability of the LCQ was assessed in those patients indicating no change (-1, 0, +1) on the GRC upon follow-up visits over 2-4 weeks. Assuming no difference in the average between the test and retest and the standard deviation of the total score is identical at each time point, 14 people were required with 0.75 as the lower limit for high agreement and 95% confidence interval (CI) in the expectation of a 0.9 intra-class correlation coefficient (ICC).5 An ICC ≥0.4 is generally regarded as a moderate correlation and >0.75 as a strong correlation.
Statistical analysis
Patients' characteristics are presented as means (standard deviation) for continuous variables and as relative frequencies for categorical variables. Spearman's correlation coefficients between LCQ scores and SF-36 scores were calculated for concurrent validity since 2 of the 3 LCQ domains did not follow a normal distribution. Internal consistency was tested by determining Cronbach's alpha coefficients for the 3 domains and the total LCQ. Repeatability was assessed by calculating the ICCs. Responsiveness was assessed using a paired t test of the LCQ scores at baseline and after clinical improvement. Statistical analysis was performed using SAS version 9.3 (SAS Institute, Cary, NC, USA).
RESULTS
Patients
In total, 207 patients were enrolled. The SF-36 data were incomplete for 5 patients. Patients' characteristics are shown in Table 1.
Concurrent validity
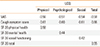
The correlation coefficients of the concurrent validity, determined in 202 patients, are shown in Table 2. The correlation coefficients between the LCQ and SF-36 varied between 0.42 and 0.58. The LCQ scores were also well correlated with the VAS and the cough symptom scores.
Internal consistency
The Cronbach's alpha coefficients for the physical, psychological, social domains, and the total questionnaire were 0.82, 0.88, 0.89, and 0.94, respectively. A Cronbach's alpha coefficient >0.7 is generally accepted as good.
Test-retest reliability
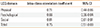
The repeatability of the LCQ in patients with no change in cough (n=23) was high, with ICCs of 0.66-0.81 (Table 3).
Responsiveness
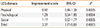
Patients who reported an improvement in cough (n=30) on follow-up visits demonstrated significant improvement in each of the domains of the LCQ (Table 4). There was a significant difference in the LCQ total score for clinically improved patients (P=0.0003) and the mean difference in the LCQ total score before and after improvements was 3.37 (95% CI: 1.71-5.03).
DISCUSSION
The Korean version of the LCQ correlated well with patients' perception as represented by the VAS and cough symptom scores, and less well with SF-36. The Korean LCQ showed a high internal consistency and appeared to be acceptably repeatable and responsive to change.
Evaluating the severity of cough is important in its clinical management. However, the evaluation of cough using validated methods remains challenging for clinicians and researchers.11 Three methods are used to assess cough severity; cough monitors used to objectively measure cough frequency, cough-specific quality-of-life questionnaires, and subjective assessments of cough severity, such as VAS.11 No current objective monitoring devices for chronic cough to guide clinicians and researchers are at present available, and the correlations between VAS and objective cough measurements or quality-of-life scores are inconsistent.11 Thus cough-specific quality-of-life questionnaires are usually recommended to assess cough severity.7,11 The LCQ is a widely used cough-specific quality-of-life questionnaire and has been shown to be repeatable and responsive, and correlates with cough frequency in chronic cough.3,4,7,12,13 The LCQ has been validated in English, Dutch and at least one other language.4,5,14
The Korean version of the LCQ correlated moderately with SF-36, which is expected since SF-36 is a measurement of generic quality of life, not specific for cough, and there could be many other components in general quality of life than cough. For the Korean LCQ, the correlation coefficients between the LCQ and SF-36 varied between 0.42 and 0.58. These results were similar with the findings of previous studies. In the developments of LCQ, Birring et al. showed moderate relationship between LCQ total score and SF-36 total score (r=0.46) and correlations between LCQ and SF36 domains were physical/role limitation due to physical problems (r=0.46), psychological/mental health (r=0.59), and social/social functioning (r=0.46).4 In the validation of Dutch version LCQ, the correlation coefficients between the LCQ (total and domain scores) and the SF-36 scale scores varied between 0.22 and 0.61.5
The Korean LCQ and patients' perception as represented by the VAS and cough symptom scores were significantly correlated. Furthermore, the Korean LCQ showed an acceptably high internal consistency and appeared to be highly repeatable and responsive to change. Thus the Korean version of the LCQ can be used to evaluate the results of interventions in the management of chronic cough, and represents a useful parameter for evaluation of chronic cough in the clinic and for research purposes.

 XML Download
XML Download