

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
For patients with progressive castration-resistant prostate cancer (CRPC) despite castration serum testosterone levels following initial androgen-deprivation therapy (ADT) for advanced prostate cancer, the therapeutic options before systemic chemotherapy, such as docetaxel, are anti-androgen withdrawal, replacement of anti-androgens, and secondary hormonal therapy [1].
After anti-androgen withdrawal syndrome in patients with CRPC, drugs for secondary hormonal manipulations include aminoglutethimide, ketoconazole, corticosteroids, and estrogenic compounds. Ketoconazole, a broad-spectrum anti-fungal agent, inhibits steroidogenesis in the testes and adrenal glands, and estramustine exerts not only non-hormonal cytotoxic effects, but also hormonal estrogenic effects. Thus, ketoconazole and estramustine serve as excellent treatment modalities in patients with CRPC [2].
Although several studies have been conducted regarding the therapeutic effects of ketoconazole and estramustine, comparisons of these treatments are limited in the literature. Thus, we investigated the efficacy, progression- free survival, and adverse effects of ketoconazole and estramustine as a secondary hormonal therapy following anti-androgen withdrawal syndrome in patients with CRPC.
MATERIALS AND METHODS
This study was conducted in accordance with the Declaration of Helsinki.
1. Study population
The medical records of 84 patients with CRPC who were treated with ketoconazole and estramustine as a secondary hormonal therapy between 2005 and 2009 were retrospectively reviewed. CRPC was defined as biochemical or radiologic progression after initial ADT, despite castration levels of serum testosterone (<50 ng/dl or 1.7 nmol/l). We considered biochemical progression as 3 consecutive increases in the PSA level at least 1 week apart, resulting in 2 increases over the nadir by 50%. Either anti-androgen withdrawal or one secondary hormonal manipulation should have been done to fulfill the criteria for CRPC. Radiologic progression included the appearance of ≥2 new lesions on bone scanning or soft tissue (nodal and visceral) lesions with use of the Response Evaluation Criteria in Solid Tumors and with lymph nodes ≥2 cm in diameter [3].
2. Data collection
Enrolled subjects were divided into 2 groups according to the drug therapy (group I: n=39, ketoconazole+prednisolone [PD] vs. group II: n=45, estramustine monotherapy). In group I, patients were administered ketoconazole (200 mg orally 3 times daily), unlike the majority of previous high-dose ketoconazole (400 mg) studies, with PD (5 mg twice daily) routinely to counteract the potential adrenal insufficiency induced by ketoconazole. Estramustine was administered orally twice a day for a total dose of 560 mg/day (group II). Patient characteristics, including age and prostate-specific antigen (PSA) level, both at the time of diagnosis and at the time the second drug was started; the Gleason score; clinical stage; prior treatment; PSA response; progression-free survival time; and adverse effects were collected for analyses.
We classified the PSA response into the following 4 categories: complete response was a PSA level below the normal baseline (4 ng/dl) for ≥4 weeks, partial response was > a 50% decrease from baseline, stable disease was a <50% decline and a 20% increase from baseline, and progressive disease was a ≥20% increase from baseline. Stable and progressive disease were considered as the nonresponse group [3].
Toxicity was graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events v4.0.
3. Statistical analysis
Student's t-test, chi-square test, and Fisher's exact test were used to compare the two groups with respect to response rates and adverse effects. Progression-free survival times were calculated and compared by using the Kaplan-Meier method and the log-rank test. A p-value <0.05 was considered statistically significant.
RESULTS
1. Baseline characteristics
The baseline median age of the entire study group of 84 patients was 72 years (range, 50 to 90 years), the median PSA level was 48.5 ng/ml (range, 1 to 3,869 ng/ml), and the median follow-up period was 4 months (range, 1 to 29 months). The Gleason score was ≥8 in 53 patients (63.1%), the clinical stage was ≥T3 in 53 patients (63.1%), and bone metastasis was present in 52 patients (61.9%). Sixty-nine patients (82.1%) previously received LHRH agonist therapy, and 15 patients (17.9%) underwent orchiectomies. The age, PSA level, Gleason score, clinical stage, and prior treatment at the beginning of secondary hormonal therapy were not statistically different (Table 1).
2. Prostate-specific antigen response rate and progression- free survival
Of the entire study group, 30 patients (35.7%) had a PSA response (complete or partial response), and 54 patients (64.3%) had no response (stable or progressive disease). The PSA response rate was higher in the estramustine group than in the ketoconazole group (37.8% vs. 33.3%); however, there was no statistical difference between the groups (p=0.672) (Table 2). Also, the PSA response rates according to Gleason score (p=0.371) and the clinical stage (p=0.839) showed no statistical difference (Tables 3, 4).
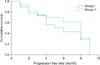
The median progression-free survival was 8 months (95% confidence interval [CI] 5.9-10.1) overall; the median progression-free survival was 5 months (95% CI 1.6-8.3) in the ketoconazole group and 8 months (95% CI 5.9-10.0) in the estramustine group. The progression-free survival was not statistically different between the groups (p=0.282) (Fig. 1).
3. Adverse effect of each drug
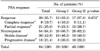
The most common side effect in the ketoconazole group was nausea and vomiting (51.3%), whereas the most common side effect in the estramustine group was anemia (77.8%). The frequency of anorexia (15 vs. 11, p=0.166) and facial edema (11 vs. 8, p=0.255) was similar in both groups, but nausea and vomiting (20 vs. 11, p=0.011) and hepatotoxicity (9 vs. 2, p=0.012) were more common in the ketoconazole group, and gynecomastia (3 vs. 15, p=0.004), neutropenia (0 vs. 9, p=0.003), and anemia (0 vs. 35, p=0.001) were more common in the estramustine group. All documented side effects were ≤grade 2 (Table 5).
DISCUSSION
In this study, there were no significant differences in PSA responses or progression-free survival between the ketoconazole and estramustine groups. The results were similar to previous studies for each drug [4-9].
Recently, the term CRPC has been used in comparison with hormone-refractory prostate cancer (HRPC), which refers to prostate cancer that has progressed or recurred after the initial hormonal ablation therapy. Distinguishing CRPC and HRPC is very important because HRPC is resistant to all hormone therapies, whereas CRPC is responsive to secondary hormone therapies such as anti-androgen withdrawal, estrogens, and corticosteroids.
Ketoconazole was originally a broad-spectrum azole anti- fungal agent that inhibits cytochrome p450 enzymes and thus inhibits androgen synthesis from steroid precursors leading to loss of adrenal steroid synthesis and testosterone synthesis by Leydig cells. Ketoconazole is commonly used with hydrocortisone because of its adrenal-suppressive effect [10]. Choi et al analyzed 11 HRPC cases in which ketoconazole (200 mg 3 times daily) and PD (5 mg 2 or 3 times daily) combination therapy was used and 10 cases in which PD monotherapy was used [4]. In the ketoconazole- PD combination therapy group, the mean PSA reduction was 23%, and the PSA decreased >50% in 27% of the patients. The mean response time was 5.2 months, which was similar to the PD monotherapy group. Wilkinson and Chodak analyzed 38 patients in whom prostate cancer progressed despite combined androgen blockade and then used intermediate-dose ketoconazole (300 mg 3 times daily) and replacement hydrocortisone [5]. Of the 38 patients, 21 (55.3%) had a PSA reduction >50%. The median time-to-progression and the median survival were 5 months and 12 months, respectively. In a prospective, randomized phase III trial, androgen-independent prostate cancer patients were targeted, and the therapeutic effect of anti-androgen withdrawal (AAWD) alone (n=132) was compared with that of simultaneous AAWD and ketoconazole (400 mg 3 times daily) plus hydrocortisone therapy (n=128) [6]. A PSA decline of >50% was observed in 11% of the patients undergoing AAWD. The median time-to-PSA progression was 5.9 months. A PSA decrease of >50% was observed in 27% of patients treated with concurrent AAWD and ketoconazole and in 32% of patients treated with ketoconazole after AAWD. The median time-to-PSA progression was 5.9 months in patients treated with AAWD alone and 8.6 months in patients treated with simultaneous AAWD and ketoconazole. According to Scholz et al, in 78 patients with high-dose ketoconazole (400 mg every 8 hours) and hydrocortisone, the median time-to-PSA progression and median survival time were 6.7 and 42.4 months, respectively [7]. A total of 34 (44 %) men had a decrease in PSA >75%. Their data indicated that a PSA decrease >75% predicted better survival than that in men with a <75% decrease.
Estramustine, a combination of estradiol phosphate and nornitrogen mustard, shows cytotoxicity by suppressing microtubules. Estramustine has toxicity similar to estrogen because the metabolite, estrogen, acts as a hormone that lowers the blood level of testosterone, leading to suppression of testosterone-sensitive tumor growth [11,12]. Han et al compared HRPC patients treated with estramustine monotherapy (n=11), estramustine and etoposide (n=12), or dexamethasone (n=10) combination therapy. The total PSA response rate was 48.5%. In the monotherapy group, etoposide combination therapy group, and dexamethasone combination therapy group, the PSA response rates were 36.4%, 41.7%, and 70.0%, respectively [8]. The overall median time-to-progression was 5 months, whereas in the monotherapy group, etoposide combination therapy group, and dexamethasone combination therapy group, it was 5 months, 5.5 months, and 5 months, respectively. The overall 1 and 2 year survival rates were 63.6% and 27.6%, respectively. Hirano et al conducted a prospective study focusing on the efficacy of estramustine phosphate monotherapy after ADT in 29 HRPC patients; in 7 (24%) patients, the PSA decreased >50%, the median duration of PSA response was 8.0 months, and the cancer- specific survival rates at 1 and 2 years were 72% and 53%, respectively [9]. The cancer-specific survival rate at 2 years was 83% in the PSA responders and 44% in the nonresponders.
In this study, 33.3% of the patients in the ketoconazole group had a PSA response, and the median progression- free survival was 5 months. In the estramustine group, 37.8% of the patients had a PSA response, and the median progression-free survival was 8 months, indicating that there was no statistically significant difference between the two groups. Furthermore, the PSA response and progression-free survival were similar to those reported in previous studies [4-9]. Because the second drugs were started at the time the disease had already progressed to CRPC, it was predictable that there would be no significant differences in the PSA response rates according to Gleason score and the clinical stage categorized at the time of prostate cancer diagnosis.
Small et al reported that 21% of ketoconazole-treated patients experienced grade 3 and 4 toxicities, including neurologic toxicity (4%), malaise or fatigue (3%), and hepatic toxicity [6]. According to Wilkinson et al, ketoconazole-related toxicity occurred in 31.6% of patients, consisting of nausea (13.2%), fatigue (10.6%), diarrhea (2.6%), visual disturbance (2.6%), and abnormal liver function tests (2.6%), and 6 (15.8%) patients discontinued ketoconazole treatment owing to intolerable side effects [5]. Estramustine commonly increases the risk of gastrointestinal problems, gynecomastia, lower extremity edema, and cardiovascular death. Estramustine can also increase the risk of thromboembolism, and in the study by Han et al, thromboembolism occurred in 6.1% of patients treated with estramustine [8]. Hirano et al reported that 15% of patients discontinued estramustine treatment due to severe gastrointestinal symptoms [9]. In this study, the common side effects reported in other studies were present, but the tolerance was relatively good, with ≤grade 2 side effects, and no patients discontinued the medication because of serious complications.
This study was not without limitations. First, besides the retrospective nature of the study and the small number of enrolled patients, we did not analyze disease-specific survival. Second, estramustine was a cytotoxic agent rather than a hormonal agent, but we used estramustine for its estrogenic effect. Third, we did not continue ADT because of Korean health insurance issues
CONCLUSIONS
Both ketoconazole and estramustine showed a PSA decline in CRPC patients before systemic chemotherapy and had mild adverse effects. Thus, either ketoconazole or estramustine can be considered as a treatment option for progressed CRPC patients after primary hormonal therapy. Ketoconazole and estramustine should be used appropriately according to the general conditions of patients and with consideration of the potential side effects of the medications. Also, we suggest that comparing ketoconazole following estramustine and estramustine following ketoconazole would be beneficial to determine optimal secondary hormone therapy in CRPC patients before docetaxel chemotherapy.




 XML Download
XML Download