

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Multilocular cystadenoma of the prostate is very rare and only a few cases have been reported. Multilocular cystadenoma of the prostate is usually misdiagnosed as a malignant pelvic tumor [1]. Although the natural history of prostatic cystadenoma remains unknown, complete surgical excision may not always be necessary [2]. Herein, we report a case of a retrovesical multilocular prostatic cystadenoma mimicking a pelvic cavity tumor.
CASE REPORT
A 58-year-old man was referred to our hospital for evaluation of elevated serum total prostate-specific antigen (PSA) 5.03 ng/ml. His medical history was unremarkable. A digital rectal examination revealed a 0.5 cm palpable nodule on the left lobe of the prostate and a soft round mass superior to the prostate. The laboratory findings were normal. Transrectal ultrasonography revealed no abnormality in the prostate and a well-defined mass located above the prostate with small cystic portions. Cystoscopic examination revealed a normal bladder and urethra. Computed tomography demonstrated a heterogeneous contrast-enhanced 6 cm mass in the retrovesical space that contained cystic and solid portions (Fig. 1). The mass was contiguous with the prostate at the lower margin, in close contact with the posterior wall of the bladder and both seminal vesicles. The tumor origin was not clear. A transrectal prostate biopsy was performed to rule out malignant disease. The biopsy showed benign prostatic hyperplasia in the prostate specimens.
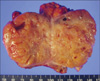
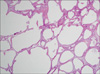
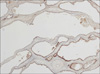
Transperitoneal laparoscopic tumor excision was performed. At surgery, a well-encapsulated solid tumor was found between the rectum and the bladder. The tumor was separated easily from the surrounding tissue, which included the bladder, prostate, rectum, and both seminal vesicles. The specimen measured approximately 7.5×5.4×2.2 cm. The cut surface of the tumor showed multiple small cysts (Fig. 2). Microscopically, the tumor was made of diffusely dilated small and large cysts. A few normal looking glands were found between the cysts (Fig. 3). The epithelial lining of the cysts were immunoreactive for PSA (Fig. 4). No atypical features or mitoses were noted in either the glandular or the stromal component of the tumor. The pathological findings were consistent with multilocular cystadenoma of the prostate.
At present, the patient has no urological complications or signs of recurrence.
DISCUSSION
Multilocular cystadenoma of the prostate is a rare, benign neoplasm consisting of prostatic glands and cysts. The age of the patients ranges from 28 to 80 years [3]. The clinical symptoms vary, but difficulty voiding and acute urinary retention are major complaints [2,4]. Serum PSA elevation and an abnormal digital rectal examination warrant a prostatic biopsy, although serum PSA does not contribute to the diagnosis of multilocular cystadenoma of the prostate [5]. Imaging studies provide useful information on a large multicystic process originating from the prostate, although a clear origin cannot always be determined. The differential diagnosis of retrovesical multilocular tumors includes an utricular duct cyst with malignant degeneration, diverticulum of the ejaculatory duct or ampulla of the vas deferens, seminal vesical cyst, simple retention cyst of the prostate, parasitic cyst from echinococcosis, primary retroperitoneal sarcoma, sarcoma of the prostate, phyllodes type of atypical prostatic hyperplasia, and multilocular cystadenoma [6].
A definitive diagnosis is made after surgical resection and by histology. According to several reports, the tumor is well demarcated and surrounded by a capsule [1-3]. Histologically, cystadenoma of the prostate consists of typical prostatic glands and cysts lined with double layers of columnar and cuboid cells with basally located nuclei with pale cytoplasm. The scattered glands have a cribriform pattern and the epithelial cells stain positively for PSA, p63, and high-molecular-weight cytokeratin.
There have been several reports of retrovesical ectopic prostate tissue [7,8]. In these cases, the clinical manifestations and imaging studies are similar to those of cystadenoma of the prostate. On histological examination, however, ectopic prostate tissue contains normal prostate epithelial layers and no cystic dilation.
In our case, we resected the tumor laparoscopically, to rule out a malignant pelvic tumor because the patient complained of no urological symptoms, but had an elevated PSA, and imaging studies revealed a solid mass apparently separated from the bladder and prostate.
In conclusion, although multilocular cystadenoma of the prostate is rare, it is needed to be considered when a solid mass with a cystic portion is seen adjacent to the prostate or bladder.

 XML Download
XML Download