

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by airflow limitation with poor reversibility and progression1. This airflow limitation is due to pathologic processes in both the airways and lung parenchyma2. The relative proportion of these two processes can vary considerably between individuals with the same degree of airflow limitation3.
Recent advances in multi-channel computed tomography (CT) scanning has allowed the quantitative assessment of both the airway and parenchymal processes. CT measurements of the extent of emphysema, airway thickening, and air trapping, as well as exercise capacity and body mass index (BMI) have been found to correlate with the severity of airflow limitation in COPD patients4-8. However, the contribution of each factor to the severity of airflow limitation has not yet been evaluated quantitatively. We therefore evaluated factors contributing the severity of airflow limitation in COPD patients quantitatively.
Materials and Methods
1. Subjects
The 213 COPD patients aged >45 years, who had smoked >10 pack-years of cigarettes, and had a post-bronchodilator forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) <0.7, but did not have bronchiectasis or sequelae of pulmonary tuberculosis were analyzed in this study.
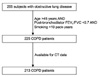
The 213 patients were selected from a group of patients with obstructive lung disease (OLD), including those with COPD, asthma and overlap syndrome (Figure 1). The 265 stable patients with OLD were recruited from the pulmonary clinics of 11 hospitals in South Korea from June 2005 to October 2008. The inclusion criteria for patients with OLD have been described elsewhere9.
All patients were evaluated by medical interviews, physical examinations, spirometry, bronchodilator reversibility tests, and lung volume and six-minute walk tests. In addition, volumetric CT was performed to evaluate airway wall thickness, emphysema severity, and mean lung density ratio at full expiration and inspiration. Multiple linear regression analysis was performed to identify the variables independently associated with FEV1, the index of the severity of airflow limitation.
Our Institutional Review Board approved analyses of the clinical and imaging data. Individual informed written consent was obtained from all patients.
2. Pulmonary function tests
Spirometry was performed using a Vmax 22 (Sensor-Medics, Yorba Linda, CA, USA) or a PFDX (MedGraphics, St Paul, MN, USA). To assess post-bronchodilator FEV1 increases, spirometry was performed pre-bronchodilation and 15 minutes after inhalation of four separate doses of salbutamol 100µg through a metered-dose inhaler (MDI) with a spacer. The post-bronchodilator FEV1 increase was expressed as the percent of the predicted normal value. Lung volumes, including total lung capacity (TLC), vital capacity (VC), functional residual capacity (FRC), and residual volume (RV), were measured by body plethysmography (V6200, SensorMedics or PFDX). Diffusing capacity for carbon monoxide (DLco) was measured by the single-breath method using a Vmax229D (Sensor-Medics) or a Masterlab Body (Jaeger AB, Würtsburg, Germany). All pulmonary function tests were performed as recommended by the American Thoracic Society (ATS)/European Respiratory Society (ERS)10-12.
3. Computed tomography
Volumetric CT scans were performed on all patients using the Somatom Sensation 16 (Siemens Medical Solutions, Forchheim, Germany), GE Lightspeed Ultra (General Electric Healthcare, Milwaukee, WI, USA), and Philips Brilliance 16 (Philips Medical Systems, Best, Netherlands) 16-slice multi-detector CT (MDCT) scanners. Patients were scanned during suspended full inspiration and expiration in the supine position without respiratory gating. Before CT scans, patients were taught how to inhale and exhale and practiced doing so under the guidance of trained nurses. The CT parameters were: 16×0.75 mm collimation, 100 eff. mAs, and 140 kVp for the Somatom Sensation 16; 16×0.625 mm, 300 mAs, 140 kVp, Pitch 0.938, and 0.5 sec/rot for the GE Lightspeed; and 16×0.75 mm, 133 mAs, 140 kVp, Pitch 1, and 0.75 sec/rot for the Philips 16. Acquired data were reconstructed using a standard algorithm with thicknesses of 0.625~0.8 mm and increments of 0.625~0.8 mm. Each CT scanner was calibrated for water using a standard water phantom monthly and after major maintenance, and for air daily. All screening scans were performed within 24 hours after calibration. Image data were stored in the Digital Imaging and Communications in Medicine (DICOM) format. Using in-house software, images of the whole lung were extracted automatically and the attenuation coefficient of each pixel was measured and calculated. The cutoff between normal lung density and a low-attenuation area (LAA) was defined as -950 HU. From the CT data, the volume fraction of the lung less than -950 HU (V950) and the mean lung density (MLD) were calculated automatically. The ratio of MLD on expiration and inspiration was calculated. The airway dimensions, wall area (WA), lumen area (LA) and wall area percent (WA%; ie, WA/(WA+LA)×100), were measured near the origin of two segmental bronchus (the right apical and left apico-posterior) selected by a consensus reading of two radiologists. The software automatically detects the airway lumen and the inner and outer boundaries of the airway wall using a full-width-half-maximum (FWHM) method13. The mean value of each segmental bronchus was used for analysis8.
4. Statistical analysis
To investigate contributors associated with airflow limitation, FEV1 was used as the dependent variable in univariate and multivariate analyses. Selected independent variables were BMI, six-minute walk distance (6MWD), smoking status (current or ex-smokers, smoking pack-years), the pulmonary function parameters TLC, FRC, RV/TLC, and DLco and the CT measurements inspiratory V950, WA%, and MLD ratio. Multiple linear regression analysis was performed to identify which variables were independently associated with FEV1. All statistical analyses were performed using the SPSS statistical package (SPSS version 12.0, SPSS Inc, Chicago, IL) and p-values <0.05 were considered significant.
Results
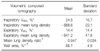
Of the 213 patients, 205 (96.2%) were men. Mean patient age was 66.3±7.3 years, mean smoking history was 46.5±25.5 pack-years, and mean FEV1 was 47.6±15.7% predicted (Tables 1, 2).
Multiple linear regression analysis showed that a significant regression model for FEV1 comprised volumetric CT measurements of MLD ratio (standardized coefficient β=-0.46; p<0.001), inspiratory V950 (%, standardized coefficient β=-0.24; p<0.001), WA% (standardized coefficient β=-0.19; p=0.001) and current smoking status (standardized coefficient β=-0.14; p=0.009) (Table 3). The model did not include BMI, total lung capacity, 6 MWD, or the other variables analyzed (p≥0.10).
Multiple linear regression analysis showed that adjusted r2 was 0.381 for volumetric CT measurements of MLD ratio, inspiratory V950 and WA%. And it showed 0.398 for CT measurements and current smoking status (Table 4).
Discussion
We have shown here that mean lung density ratio, inspiratory V950, and wall area %, as evaluated by volumetric CT, as well as current smoking status were significant contributors of FEV1 in COPD patients. This finding indicates that the severity of airflow limitation could be, in part, determined by imaging measurements of the airway and emphysema.
Structural changes, as assessed by CT scanning, have been reported to correlate with the severity of airflow limitation7,14-16. In these previous reports, the structural changes included extent of emphysema, as evaluated by low attenuation area (equivalent to V950 in this study), and abnormalities of large airway walls, as evaluated by wall thickness (equivalent to wall area % in this study). In addition, comparison of CT scans at expiration and inspiration was reported to reflect small airway diseases17,18. To assess the extent of small airway disease in 34 COPD patients, we developed a CT air-trapping index (mean lung density ratio) by comparing the mean lung density seen on CT scans at full expiration and inspiration8. The results presented here also show that mean lung density ratio is the most significant contributor of the severity of airflow limitation in these patients. This finding is consistent with results showing the importance of small airway disease in the pathogenesis of COPD6,19. Although obstruction of the smaller airways has been found to correlate with the severity of airflow limitation7, to date there have been no accurate CT-based measurements of small airway lesions in COPD patients. We have previously shown that mean lung density ratio correlated with the physiologic air-trapping index (vital capacity-FVC) and FEV18. The results presented here validate the importance of mean lung density ratio, although it has not yet been confirmed as directly reflecting small airway disease.
Emphysema severity and airway wall thickness, as determined by CT scans, have also been found to correlate with FEV120-23. Our findings confirm these results, in that we found that emphysema severity and large airway wall thickness, as measured by CT scan, could contribute airflow limitation. Cigarette smoking, the major risk factor for COPD, causes abnormalities by inducing inflammation in the lung parenchyma and airways. Indeed, we found that current smoking status was an independent contributor of FEV1 in COPD patients, whereas smoking history, as assessed by pack-years, was not. Although the amount of previous smoking is related to the severity of COPD, it may not be an independent predictor of FEV1 after correction for the morphologic changes of the airway and emphysema that are thought to result from smoking.
Our multiple linear regression analysis did not include BMI, total lung capacity or 6 MWD, indicating that the contributions of these factors to FEV1 may not be independent but may be indirectly influenced by the morphologic changes measured by CT scans.
Although we evaluated FEV1 as the dependent variable for contributing the severity of airflow limitation, it has been suggested that the severity of airflow limitation be evaluated by post-bronchodilator FEV1 in COPD patients24. Repeat multiple linear regression analysis using post-bronchodilator FEV1 as the dependent variable resulted in a similar regression model, with mean lung density ratio (standardized coefficient β=-0.44; p< 0.001), inspiratory V950 (%, standardized coefficient β=-0.30; p<0.001), wall area% (standardized coefficient β=-0.16; p=0.003) and current smoking status (standardized coefficient β=-0.15; p=0.006) being independent contributors of post-bronchodilator FEV1.
This study had several limitations. First, the mean lung ratio measured by volumetric CT may not completely reflect small airway disease. We have not shown a direct correlation between mean lung ratio and the severity of small airway disease in COPD patients. A direct correlation needs to be assessed by the pathologic or pathophysiologic evaluation of small airway disease, in accordance with changes in mean lung density.
Another limitation was that our study subjects were predominantly male smokers, either present or past. The high proportion of males in our study may be due to the high prevalence of male smokers and very low prevalence of female smokers in Korea. As there may be gender differences in COPD25,26, further investigations are warranted.
In conclusion, we found that mean lung density ratio, emphysema severity, and airway wall thickness, as measured by volumetric CT, as well as smoking status, could contribute the severity of the airflow limitation in patients with COPD.



 XML Download
XML Download