

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cervical cancer is the second most common gynecologic cancer worldwide, accounting for 13% of all female cancers in developing countries [1]. In Thailand, cervical cancer is the most common gynecologic cancer with the incidence rate of 29.2 per 100,000 women per year, and is also the most common cause of death with the mortality rate of 15.2 per 100,000 women per year [1]. Cervical cytologic screening has an important role in early detection of pre-invasive or invasive cervical lesions which usually have excellent treatment outcomes, therefore, resulting in reduced mortality rate.
The Bethesda system [2] has categorized abnormal cervical cytology of squamous epithelium into atypical squamous cells (ASC), low grade squamous intraepithelial lesions (LSIL), high grade squamous intraepithelial lesions (HSIL), and squamous cell carcinoma (SCC). HSIL and SCC generally have high risk of underlying histopathology of high grade lesions (HGL) including CIN 2-3 and invasive cancer requiring definite investigation and management. Unlike HSIL and SCC, ASC and LSIL usually represent low risk pathology e.g., reactive/inflammation or low grade lesions (LGL) including cervical intraepithelial neoplasia (CIN) 1 and human papillomavirus (HPV) that can expectant management. However, both ASC and LSIL also have definite risk of harboring HGL albeit at much lower rates than HSIL or SCC. The incidence of HGL varies in ASC according to its subtypes of ASC: ASC, of undetermined significance (ASC-US) and ASC, cannot exclude HSIL (ASC-H). For ASC-US, the incidence of CIN 2-3 and SCC ranged from 2-13% and 0-2%, respectively [3-6]. These incidences are much higher for ASC-H and LSIL. The CIN 2-3 and SCC could be identified in 25-75% and 0-8% of ASC-H respectively [7-9], and in 15-41% or up to 5% of LSIL [10-13].
The American Society for Colposcopy and Cervical Pathology (ASCCP) [14] has recommended triage management of ASC-US. HPV-DNA testing is more preferred than other two alternatives [8,15]. However, HPV testing may not be practical in low resource settings including some areas of Thailand due to its high cost and requirement of high technology to process the test. A follow-up cytology test will make women anxious and some may have a poor compliance for a follow-up visit. Colposcopy, as another one option, requires experienced operators who are limited in numbers, leading to a long waiting time. With these restrictions added with the possibility of HGL in women with ASC or LSIL, a simple cost-effective means to identify HGL will be useful. Particularly in a very limited resource, any other means to screen and probably to treat women with suspicious lesions in the same setting might be ideal. Among these, visual inspection with acetic acid (VIA) is probably the most common method. Many studies reported achievement of VIA as a primary screening test [16-21].
The advantages of the VIA are its low cost, being able to be carried out by trained paramedical personnel, and a relatively high sensitivity. The sensitivity to detect HGL ranged from 61 to 100% [20-25] while the specificity, positive predictive value (PPV), and negative predictive value (NPV) were 36-98% [20-25], 9-44% [19,22,23,26], and 88-100% [19,22,23,26], respectively. Another obvious benefit is its immediate results from the clinical impression leading to a proper counselling and a possibility of the "see and treat" approach. This certainly can reduce the problem of a loss to follow-up which is especially common in an outreached area. The main limitation is false-positive results from the VIA which may lead to overtreatment.
We aim to evaluate the value of VIA as an intermediate test to detect any HGL for women with ASC or LSIL cervical cytology from Pap smear. This will add information to guide for a clinical practice particularly in settings which have limited resources as in some areas of our country as well as other countries with similar financial background or limited availability of health service sectors.
MATERIALS AND METHODS
This study was conducted after approval by an ethics committee of the institution. Inclusion criteria were women who had cervical cytologic diagnoses of ASC or LSIL and were scheduled for colposcopic examination at gynecologic oncology out-patient clinic at Faculty of Medicine Vajira Hospital from July 1, 2010 to February 28, 2011. Women who had history of cervical cancer or pre-invasive cervical lesions, had hysterectomy, were pregnant, or had an incomplete medical record were excluded.
Sample size was obtained based on 83% sensitivity of VIA to detect HGL in prior report [24] and maximum allowable error of 15%. With an α error of 5% and the prevalence of HGL in ASC and LSIL Pap smear of 25% (statistical data of the institution in the past 3 months), sample size of 106 women was required.
In a standard colposcopic procedure, the cervix was examined under colposcopic examination by a gynecologic oncologist or fellows in training for any lesions especially abnormal vascular pattern before an application of 3-5% acetic acid. For a woman with satisfactory colposcopic examination (all transformation zone was totally visualized), any acetowhite areas were biopsied for histopathologic examination (colposcopic directed biopsy [CDB]). In any case of unsatisfactory colposcopy or there was no gross ectocervical abnormality, an endocervical curettage (ECC) would be carried out. Women who had satisfactory colposcopy with no suspicious lesions over ecto and endo-cervices were defined as "normal colposcopy" and were schedule for a follow-up Pap smear.
In our study to evaluate the clinical performance of the visual inspection of cervix after application of acetic acid or so called "Visual Inspection with Acetic Acid or VIA" test, every woman was informed that the procedure is a crucial step in routine colposcopic examination. One of the researchers (MP), who had been well trained and was skilled in colposcopic procedure, performed a careful inspection of the cervix by naked-eyes after acetic acid application. The sites and characteristics of the lesions were mapped and the diagnosis of the VIA test before proceeding to the next step of investigation. The VIA results were interpreted as positive or negative by using the criteria of the International Agency for Cancer Research [27]. The standard colposcopic examination and appropriate investigations were proceeded by another gynecologic oncologist blinded to the findings from the VIA tests. Management for the women was provided according to the results of a primary histologic diagnosis from tissue biopsy obtained by CDB and/or ECC. Women with normal or inflammatory histology or lesion of CIN 1 were scheduled for a follow-up cytology. Any women with lesions of CIN 2-3 or worse were classified as HGL and would undergo cervical conization by loop electrosurgical excision procedure (LEEP) or cold knife conization as appropriate. Hysterectomy was performed as indicated by the severity of lesions identified from the conization specimen or other associated gynecologic pathologic findings.
Clinical and pathological data of the women were retrieved from the out-patient charts and the archives of the Anatomical Pathology Department. Data collected were: age, menopausal status, marital status, parity, cervical cytology, the result of VIA test, and the definite cervical histology. Histopathology referred to the most severe histologic diagnosis from CDB, ECC, LEEP, or hysterectomy. Data were analyzed by parametric and nonparametric statistics, using SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used for demographic data and summarized as frequencies, percentages, means with standard deviation, or median with ranges. Differences between variables were evaluated with the chi-square or Fisher-exact test as appropriate. The primary outcome was considered significant only if the p≤0.05.
The diagnostic values of VIA test including sensitivity, specificity, positive predictive value, and negative predictive value were determined by comparing the results of the VIA test and the final histopathology which was used as the gold standard. HGL, which had clinical impact requiring prompt management, was set as a cut-off point of reference.
RESULTS
During the study period, 6,261 women had cervical cytologic Pap smear in our institute. Cytologic diagnosis of ASC was identified in 66 women (1.1%) and LSIL in 65 (1.1%). From 131 women, 25 were excluded due to: history of pre-invasive cervical lesions and cervical cancer (15 women), had prior hysterectomy (6 women), were pregnant (two women), and were lost of follow-up after cervical tissue biopsies (two women). A total of 106 women with ASC or LSIL cytology met all inclusion criteria and were included in the study. Mean age of the women was 38.4±12.8 years. Majority of the women were premenopausal and multiparous, with a median parity of 1.6 (range, 0 to 8). Median interval time from Pap smear until VIA and colposcopy was 6.8±3.4 weeks (range, 1.9 to 19.9 weeks). There were 55/106 (51.9%) women with cytologic diagnosis of ASC and 51/106 (48.1%) with LSIL.
The clinical characteristics of the women in the study are shown in Table 1. Nearly half of the women (49.1%) who had ASC or LSIL were asymptomatic and had Pap smear test as a general health screening. Among women who had symptoms and sought for medical consultation, abnormal vaginal discharge and pelvic pain were the two common complaints (15.1% for each).
From all 106 women included in the study, the VIA test was interpreted as positive in 33 women (31.1%) and negative VIA in 73 women (68.9%). From colposcopic examination, 75 (70.8%) had satisfactory colposcopy while 31 women (29.2%) had unsatisfactory results. Thirteen women had no suspicious lesions from the colposcopic examination and were scheduled for follow-up Pap test at 6 months. CDB or ECC were performed in 76 (71.7%) and eight women (7.5%) respectively. Nine women (8.5%) had both CDB and ECC in the same setting. Thirteen women subsequently underwent LEEP based on the primary histologic diagnosis from biopsy or ECC as CIN-2 (seven cases) or CIN-3 (six cases). One woman who was found from LEEP specimen to have early stromal invasion (2 mm) ultimately had simple hysterectomy as well as the other three women who had biopsy results of only CIN-1 but had co-incidental pathology of myoma uteri or adenomyosis.
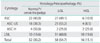
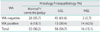
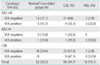
From 106 cases with cytologic diagnoses of ASC or LSIL, normal colposcopy and unremarkable histology/histopathology (negative for malignancy, endocervical polyp, or cervicitis) were found in 32 women (30.2%) while CIN 1 was found 58 women (54.7%). Aside from one case with invasive cancer, HGL or CIN 2-3 was found in 15 women (14.2%). The histology/histopathology of women with ASC and LSIL in our study are shown in Table 2. Among the 33 women with VIA test positive, 14 had HGL (42.4%) while 19 had no significant lesions (false positive cases, 57.6%): no pathology (one case), cervicitis/polyp (five cases), or CIN-1 (13 cases). From 73 women with VIA test negative, only two (2.7%) had HGL (false negative cases, 2.7%); both of them had histopathology of CIN 2. Other negative VIA cases had negative pathology (17 cases), only cervicitis (8 cases), or CIN-1 (27 cases). Table 3 shows histology/histopathology of women according to the VIA results.
When we evaluated the histopathology of women according to their cytology stratified by the VIA results. We found that women who had higher degree of abnormal cytology (from ASC-US to ASC-H to LSIL) and VIA positive were directly associated with HGL. Histology/ histopathology of women according to their cytology and VIA test are shown in Table 4.
The diagnostic values of VIA using HGL as the cut-off level; the sensitivity, specificity, positive predictive value, and negative predictive value with their 95% confidence intervals were 87.5% (81.2-93.8%), 78.8% (71.1-86.7%), 42.4% (33.0-51.8%), and 97.2% (94.2-1.0%), respectively.
DISCUSSION
During the study period, the prevalence of either ASC or LSIL in our institute was 1.1% (for each) which was in the ranges as had been reported in other studies from 1.0-4.5% [3,28,29] and 0.3-1.6%, [13,28,29] respectively.
The prevalence of ASC and LSIL during the limited study period of our study was concordant to our prior reports by Limpvanuspong et al. [3] and Khuakoonratt et al. [13] who identified 1.7% prevalence of ASC (830/46,680 women who had Pap smear from 2003 to 2006) and 0.9% LSIL (691 from 72,087 women from 2001 to 2005). Both studies evaluated the rates of HGL and cancer in women with cervical cytology of ASC or LSIL. One demonstrated 9.1% of HGL and 0.9% invasive cancer from 287 women with ASC [3] while another found 15.0% HGL and 1.3% invasive cancer from 226 women who had LSIL [13]. Since the majority of ASC or LSIL has a final histologic diagnosis of only LGL, an immediate investigation or treatment may be delayed. Submitting all women with low risk cytologic diagnoses (ASC, LSIL) to colposcopy may not be possible or inconvenient. This is especially true in a scenario when the number of colposcopists is limited and the privilege must be given to the more severe cytologic lesions. Nevertheless, because of the real existence of HGL in these ASC and LSIL, other means such as VIA to exclude HGL is a reasonable alternative option. The advantages of VIA are low cost, real time result, and can be achieved by trained paramedical workers. These render it suitable in low resource areas. Few studies used VIA in adjunct with the Pap test as a screening test to detect HGL, sensitivity of the two combined methods was improved compared to Pap test only [23,30].
Prevalence of positive VIA test depends on the characteristic of the population studied e.g., asymptomatic women or symptomatic; co-incidental pathology of cervical dysplastic lesions and cervicitis or inflammation; cervical anatomy or area of transformation zone which is affected by age or menopausal status; or parity [31]. We found VIA positive in 33% which was higher than 10-16% reported in other studies which generally used VIA as an alternative option for primary screening test in the general normal population [32]. This was because our study evaluated VIA in a different setting, as the secondary test in women with mild cytologic abnormalities of ASC and LSIL.
A few meta-analysis reports including several studies of VIA found various diagnostic performances of VIA [33-35]. The sensitivity and the specificity of VIA ranged from 72-84% and 79-85%, respectively. The differences might lie with the subjects studied (with or without gynecologic symptoms), different thresholds, or different confirmatory diagnostic tests. One recent meta-analysis by Sauvaget et al. [36], including only studies with histologic confirmation, reported high diagnostic performance of VIA to detect cervical lesions using HGL as the threshold [36]. The sensitivity of VIA for cervical cancer screening was 80% while the specificity was 92%. Since all of their reviewed studies were intended for screening in asymptomatic women, the PPV demonstrated in this review was only 10% [36]. The authors found that the region or place of screening, study period, size of study population, and capacity of the screeners (health worker, nurse or physician) had no effect on VIA accuracy. In our study, VIA as a subsequent test in ASC and LSIL cytology to detect HGL had high sensitivity and NPV at 87.5% and 97%, respectively. Only two cases (with cytologic diagnosis of ASC-US and LSIL) had false-negative VIA. The final histology was only CIN 2. While all cases with HGL including the one case of invasive cancer (with ASC-H cytology) which had positive VIA. As we found the prevalence of HGL was higher in women with higher degree of cytologic abnormalities especially when the VIA test was positive, special attention to look for HGL is warranted in these subgroups.
From previous studies, the false-positive VIA results were due to inappropriate light source, an inadequate trained or experience of the observer, and the presence of cervical inflammation/infection or metaplasia [21]. These factors may lead to an overtreatment if a see and treat policy is applied. Our setting for the VIA test is considered as optimal, yet, the false positive rate in our study was high at 58% (19 cases). Approximately 15% of these false positive cases had inflammation/polyps while 39% had CIN 1 (Table 3). Aside from the former group with obvious inflammation which can cause a false positive VIA, we did not know whether the latter group of CIN 1 also had associated metaplasia/inflammation or the dysplastic lesion itself can cause positive VIA. For any reasons, these conditions should be aware of, especially in a circumstance of the see and treat approach.
With the high sensitivity and specificity of VIA test in ASC and LSIL to detect HGL found in our study, this may serve as an intermediate test in women with mild abnormal Pap smear of ASC or LSIL. Women who are not at high risk for HGL (ASC or LSIL with negative VIA test) may undergo a follow-up Pap test while the women who are at high risk (ASC or LSIL with positive VIA test) must directly have colposcopy. The reduced number of women who must undergo colposcopic examination may be practical in settings when the women decline or not ready for a referral at the moment, where there is no or only limited number of colposcopists, and when HPV-DNA testing is not possible. Further studies in more numbers of women will definitely confirm the safety of this alternative option in women with abnormal Pap smears.

 XML Download
XML Download