

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The aim of this study was to determine how well multi-detector computed tomography (MDCT) scans predict the need for a laparotomy in patients with anterior abdominal stab injuries.
Materials and Methods
Eighty patients with abdominal stab injuries who underwent MDCT scans were enrolled. MDCT was performed to identify active bleeding and injured organs and to assess the accuracy between MDCT and the laparotomy findings. MDCT was considered positive or negative with respect to the need for an exploratory laparotomy. The diagnostic performance of MDCT for identifying the need for laparotomy was estimated.
Results
MDCT predicted bowel and mesentery injuries in 31 of 80 patients and 28 patients were truly positive. MDCT predicted active bleeding in 23 of 80 patients and 19 patients had active bleeding. MDCT predicted the need for laparotomy in 43 of 80 patients. A laparotomy was performed in 55 of the 80 patients and 42 were therapeutic. Overall, a MDCT scan predicted the need for laparotomy with 95% sensitivity, 92% specificity, and 93% accuracy.
Figures and Tables
Fig. 1
Stab wound to anterior abdomen in a 43-year-old man.
A. CT scan shows defect (thin arrow) in anterior abdominal wall. Hematoma in both paracolic gutter (thick arrows) with contrast material extravasation (arrowhead) in the mesentery is seen.
B. Lower section of the CT scan of the same patient shows bowel wall thickening (black thin arrow) and free intraperitoneal air (white thin arrows). Also seen is streaking of the mesenteric fat adjacent to the thickened bowel (white arrowhead). An injury to the mesenteric vessel and ileum was confirmed surgically.
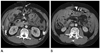
Fig. 2
Stab wound to anterior abdomen in a 25-year-old man. CT scan shows defect (thin arrow) in anterior abdominal wall. Free intraperitoneal fluid in mesentery and right paracolic gutter (thick arrows) with linear contrast material extravasation (arrowhead) along right side anterior abdominal wall is seen. No free intraperitoneal air is seen on CT scan. At surgery, an injury to the mesenteric vessel was seen and no bowel injury was found.
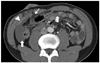
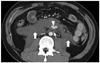
Fig. 3
Stab wound to anterior abdomen in a 33-year-old man. CT scan shows large mesenteric hematoma (thick arrows) including contrast material extravasation (arrowhead) adjacent inferior mesenteric artery (thin arrow). At surgery, transection of proximal inferior mesenteric artery was found.




References
1. Shaftan GW. Indications for operation in abdominal trauma. Am J Surg. 1960. 99:657–664.
2. Shanmuganathan K, Mirvis SE, Sover ER. Value of contrast-enhanced CT in detecting active hemorrhage in patients with blunt abdominal or pelvic trauma. AJR Am J Roentgenol. 1993. 161:65–69.
3. Rizzo MJ, Federle MP, Griffiths BG. Bowel and mesenteric injury following blunt abdominal trauma: evaluation with CT. Radiology. 1989. 173:143–148.
4. Dowe MF, Shanmuganathan K, Mirvis SE, Steiner RC, Cooper C. CT findings of mesenteric injury after blunt trauma: implications for surgical intervention. AJR Am J Roentgenol. 1997. 168:425–428.
5. Adams DB. Mandatory exploration for penetrating abdominal wounds. Arch Surg. 1991. 126:115.
6. Nance FC, Cohn I Jr. Surgical judgment in the management of stab wounds of the abdomen: a retrospective and prospective analysis based on a study of 600 stabbed patients. Ann Surg. 1969. 170:569–580.
7. Nance FC, Wennar MH, Johnson LW, Ingram JC Jr, Cohn I Jr. Surgical judgment in the management of penetrating wounds of the abdomen: experience with 2212 patients. Ann Surg. 1974. 179:639–646.
8. McAlvanah MJ, Shaftan GW. Selective conservatism in penetrating abdominal wounds: a continuing reappraisal. J Trauma. 1978. 18:206–212.
9. Leppäniemi AK, Voutilainen PE, Haapiainen RK. Indications for early mandatory laparotomy in abdominal stab wounds. Br J Surg. 1999. 86:76–80.
10. Salim A, Sangthong B, Martin M, Brown C, Plurad D, Inaba K, et al. Use of computed tomography in anterior abdominal stab wounds: results of a prospective study. Arch Surg. 2006. 141:745–750. discussion 750-752.
11. Biffl WL, Kaups KL, Cothren CC, Brasel KJ, Dicker RA, Bullard MK, et al. Management of patients with anterior abdominal stab wounds: a Western Trauma Association multicenter trial. J Trauma. 2009. 66:1294–1301.
12. Soto JA, Morales C, Múnera F, Sanabria A, Guevara JM, Suárez T. Penetrating stab wounds to the abdomen: use of serial US and contrast-enhanced CT in stable patients. Radiology. 2001. 220:365–371.
13. Sherck J, Shatney C, Sensaki K, Selivanov V. The accuracy of computed tomography in the diagnosis of blunt small-bowel perforation. Am J Surg. 1994. 168:670–675.
14. Dauterive AH, Flancbaum L, Cox EF. Blunt intestinal trauma. A modern-day review. Ann Surg. 1985. 201:198–203.
15. Fakhry SM, Brownstein M, Baker CC, Watts DD, Oller D. Relatively short diagnostic delays produce morbidity and mortality in blunt small bowel injury (SBI): an analysis of time to operative intervention in 202 patients from a multicenter experience. J Trauma. 1999. 47:207.
16. Demetriades D, Rabinowitz B. Indications for operation in abdominal stab wounds. A prospective study of 651 patients. Ann Surg. 1987. 205:129–132.
17. Chiu WC, Shanmuganathan K, Mirvis SE, Scalea TM. Determining the need for laparotomy in penetrating torso trauma: a prospective study using triple-contrast enhanced abdominopelvic computed tomography. J Trauma. 2001. 51:860–868. discussion 868-869.
18. Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL, Scalea TM. Triple-contrast helical CT in penetrating torso trauma: a prospective study to determine peritoneal violation and the need for laparotomy. AJR Am J Roentgenol. 2001. 177:1247–1256.
19. Ramirez RM, Cureton EL, Ereso AQ, Kwan RO, Dozier KC, Sadjadi J, et al. Single-contrast computed tomography for the triage of patients with penetrating torso trauma. J Trauma. 2009. 67:583–588.
20. Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL, Hogan GJ, Scalea TM. Penetrating torso trauma: triple-contrast helical CT in peritoneal violation and organ injury--a prospective study in 200 patients. Radiology. 2004. 231:775–784.
21. Tsang BD, Panacek EA, Brant WE, Wisner DH. Effect of oral contrast administration for abdominal computed tomography in the evaluation of acute blunt trauma. Ann Emerg Med. 1997. 30:7–13.
 XML Download
XML Download