

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
It is well established that rheumatoid arthritis (RA) is associated with increased cardiovascular (CV) morbidity and mortality (12). In the general population loss of proteins within the urine shows a strong and continuous association with CV risk (3). Therefore, quantification of urinary albumin excretion can help to detect individuals with an increased CV risk (4). Of note, there are only few data on urinary albumin excretion in RA patients.
The common term "microalbuminuria" (MA) is somewhat arbitrary and defines patients with an albumin excretion – if a spot sample is used – of 30 to 300 mg/g in the urinary albumin-creatinine ratio (ACR) (5). Historically, MA was initially recognized as it is an important factor in the diagnosis of early renal damage. Especially in the presence of diabetic nephropathy determination of urinary albumin excretion is of relevance as it can be recognized well before the glomerula filtration rate starts to decline. However, when appreciating MA as a marker of CV risk it is of outstanding importance to keep in mind that low levels of albuminuria – well below the usual definitions for MA – also are associated with an increased CV risk (67). Given the fact that the CV risk represents a continuum and, in addition, urinary albumin excretion is dependent on factors such as age, race and body composition, a dichotomous differentiation according to a given cut-off ("MA present" vs. "MA not present") is unlikely to properly reflect the underlying pathophysiology as well as its associated risk (8).
Previously we could demonstrate that RA patients have an increased augmentation index (AIx) (9), a marker of vascular dysfunction and CV risk, and that this increase is independent of the presence of traditional CV risk markers (10).
Aim of the present study was to investigate whether urinary albumin excretion is increased in RA patients as compared to controls not having RA (n-RA group). As urinary albumin excretion is frequently seen in diabetic patients we also measured urinary albumin excretion in such patients and related the findings to RA patients. In addition, we evaluated whether urinary albumin excretion is associated with vascular dysfunction as assessed by pulse wave analysis.
MATERIALS AND METHODS
Patients
Included in the present study were patients with a diagnosis of RA according to the 1987 American College of Rheumatology criteria (11).
A total of 341 participants were included in the study. Of these, 215 were diagnosed with RA. Patients in the RA group and in the n-RA group both were recruited from our inpatient as well as from the outpatient clinic. Given the fact that the department is an Internal Medicine department with several subspecialties this is also reflected in the present study population. However, patients with previously diagnosed kidney disease as well as patients with urinary tract infection were excluded from this study. In addition, patients with other acute infectious diseases (e.g., respiratory tract, skin, gastrointestinal, etc.) and/or arrhythmia, which preclude measurement of AIx, were excluded. For each participant co-morbidities and traditional CV risk factors were registered. The diagnosis of diabetes (DM) was based either on the Guidelines of the Austrian Diabetes Association (12) or on whether the patient currently had any form of antidiabetic treatment. Smoking habits, antihypertensive medication and a history of prior CV events were registered as provided directly by the study participants and as determined by evaluation of the medical records. A family history of premature coronary heart disease was judged to exist if coronary heart disease was evident in a male first-degree relative <55 years of age or in a female first-degree relative <65 years of age (13).
In RA patients we evaluated disease duration, treatment with disease modifying anti-rheumatic drugs (DMARD) and the presence of rheumatoid factor. Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and patient global assessment (PGA; 100 mm visual analogue scale) were measured. In addition, tender joint count (TJC; 28 joints), swollen joint count (SJC; 28 joints) and the disease activity score 28 (DAS 28) were determined (14). Remission was defined as a DAS 28 <2.6, low disease activity as ≥2.6 and ≤3.2, moderate activity as >3.2 and ≤5.1 and high activity as a DAS 28 >5.1 (14).
Urinary albumin and creatinine were measured with Cobas 8000 c module (Roche Diagnostics, Vienna) and the ACR (15) was calculated. If the urinary albumin excretion was undetectably low the ACR was set to 0, in order to be able to also use these cases for further calculations. In the statistical clustering process (see section "Statistical analysis") these cases had to be excluded due to theoretical assumptions on properties of the underlying distributions.
Pulse wave analysis
Pulse wave analysis (PWA) was performed as described previously on the radial artery using applanation tonometry with a high-fidelity micro-manometer (SPC-301, Millar Instruments, Houston, TX, USA) (9). In short, the aortic pressure waveform was derived from radial tonometry using a previously validated generalized transfer function relating radial to aortic pressure waveform in the integrated system software of the Sphygmocor apparatus (AtCor Medical, version 6.31, Sydney, Australia) (1516). To exclude the influence of heart rate on the AIx, the normalized index for 75 beats per minute was used (17). Only high-quality data were used for the analyses. Each measurement was taken twice and the mean used for statistical analysis. After the patient had lain supine for a minimum of five minutes (18), blood pressure was recorded immediately before PWA using an automated oscillometric method (boso medicus, Bosch + Sohn GMBH, Jungingen, Germany; validated and certified by the German Society for Hypertension).
Statistical analysis
For comparison of continuous variables between the groups the Mann-Whitney U-test was used. For comparison of indicator variables between the groups the chi-square test was used. For correlation of continuous variables within a group the Kendall tau rank correlation coefficient was calculated. For the presentation of the ACR, which is substantially right skewed, the median is given and as a measure of spread the interquartile range (IQR) is presented (1st quartile subtracted from the 3rd quartile).
We calculated ACR for the RA group and the n-RA group. In addition, we divided our patients into 4 ordered categories: 1: no RA and no DM (RA-/DM-, n=74), 2: RA, but no DM (RA+/DM-, n=195), 3: no RA, but DM (RA-/DM+, n=52), and 4: RA and DM positive (RA+/DM+, n=20).
For further statistical analysis 15 zero-values (ACR) in total had to be excluded from the general sample which led to a sample-size-reduction in the ordered groups as follows: 1: no RA and no DM (RA-/DM-, n=72), 2: RA, but no DM (RA+/DM-, n=185), 3: no RA, but DM (RA-/DM+, n=51), and 4: RA and DM positive (RA+/DM+, n=18).
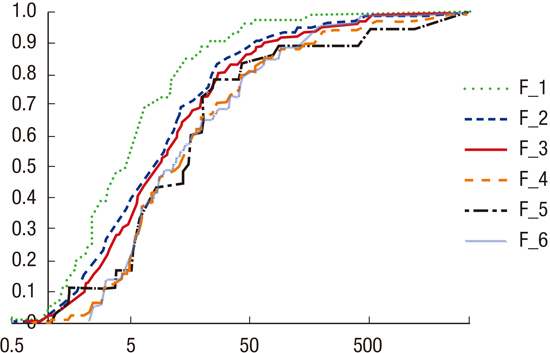
We used (empirical) cumulative distribution functions (CDF) for the analysis of urinary albumin excretion. The two-sided Smirnov test statistic for testing on equality of continuous distributions estimates some sort of normed "distance" of two empirical CDFs which in this context depicts the dissimilarity of the distributions of the underlying random variables. This approach was used to answer the following questions: Is it possible to
To achieve this, we calculated the Smirnov test statistic matrix of the ordered groups' samples in a stepwise approach, identifying the two groups corresponding to the minimum matrix entry and joining them to a new group. This procedure was repeated as long as the minimum entry is smaller than the 0.99-quantile of the Kolmogorov distribution (namely 1.628). Finally, the difference between distributions of resulting groups was investigated.
RESULTS
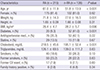
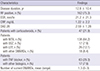
In a total of 341 patients the ACR was analysed (215 in the RA group, 126 in the n-RA group). Demographic characteristics for both patient groups are given in Table 1. In Table 2 further characteristics of the RA group are provided. ACR showed a substantially right-skewed distribution in both groups. In the RA group the median ACR was 6.6 mg/g (range 0 to 3,469.4 mg/g, IQR 2.7 to 19.4 mg/g). In the n-RA group the median was 5.7 mg/g (range 0 to 1,708 mg/g; IQR 2.4 mg/g to 16.1 mg/g). Without further adjustment there was no significant difference in medians between the RA and n-RA group.
In the following the distinct groups RA-/DM-, RA+/DM-, RA-/DM+, and RA+/DM+ were investigated. In the first step the smallest Smirnov test statistic corresponded to groups 3 and 4 (and is equal to 0.477, i.e. smaller than 1.628). Therefore, groups 3 and 4 were joined to a new group 5. In the second step the smallest statistic corresponded to groups 2 and 5 (equal to 1.5). Therefore, groups 2 and 5 were joined to a new group 6. In the next step the test statistic (1.869) exceeded 1.628 and, therefore, groups 1 and 6 may not be joined further. Thus, the initial classification of the patients into the four groups could be reduced to the two groups 1 (no RA and no DM) and 6 (either RA or DM or both). In Fig. 1 the CDF of each of the six samples are plotted using a logarithmically scaled abscissa. Fig. 1 demonstrates that F_1 is lying "more to the left" than F_6. This demonstrates that ACR in group 1 is smaller than in group 6. Therefore, patients without RA and without DM have a significantly lower ACR than patients suffering from either RA or DM or both (one-sided Smirnov test; P<0.001). Fig. 2 shows a boxplot of ACR for groups 1 and 6, where the median of ACR is significantly lower in group 1 (4.5 mg/g) compared to group 6 (8.1 mg/g).
Table 3 gives the results of the PWA. Using Kendall's tau we could not find a correlation between ACR and AIx (r=0.04).
DISCUSSION
It is well established that increased urinary albumin excretion predicts all-cause and CV mortality (19). Initially, urinary albumin excretion was recognized as a predictor of overt kidney disease in patients with diabetes (20). However, in the following it became evident that urinary albumin excretion is also a predictor of decline of glomerular filtration rate in non-diabetic patients (21) and, going further, that a decline of GFR in diabetic nephropathy can occur even in the absence of MA (2223). In addition, increased urinary albumin excretion is associated with a number of conditions which in turn are contributors to CV disease, such as hypertension, obesity, insulin resistance, dyslipidemia and inflammatory conditions (24). Thus, the debate exists whether – and if yes, to what extend – increased urinary albumin excretion should be regarded as a marker of kidney disease or rather as a marker of microvascular injury (25).
In the present study in the RA group the median ACR was 6.6 mg/g and in the n-RA group the median was 5.7 mg/g. This analysis, however, did not take DM into account. By further categorising patients according to their RA and DM status a more detailed analysis was possible. In general, all 4 patient groups (F_1–F_4) showed a similar – right-skewed – ACR distribution. However, from the plot it is evident that in F_1 (RA-/DM-) the number of patients with an increased ACR is lower compared to the other groups. Thus, this group 1 differs from the other groups. Using complete-linkage-clustering revealed that two separate clusters of patients exist: on the one hand, healthy individuals (F_1, RA-/DM-), and on the other hand patients with either RA or DM or both (F_2–F_4). These analyses demonstrate that – even if there is substantial overlap between the groups and the distribution of ACR is strongly right-skewed – patients without RA and without DM have lower urinary albumin excretion compared to patients with either RA or DM or both.
While it seems evident that urinary albumin excretion is associated with CV risk (26) it is much less clear what pathophysiologic mechanisms are contributing. During physiologic conditions up to 2 g albumin per day are filtered at the glomerula in the kidneys. About 99% are reabsorbed at the tubular level. Finally, only approximately 7 mg per day are excreted within the urine (25). Under physiologic conditions a sophisticated and incompletely understood interplay between the glomerular basement membrane, the podocyte and the endothelium prevents the loss of proteins at the level of the glomerulum (27). In the case of injury of one of these components much larger amounts of albumin are filtered, thereby exceeding the reabsorption capacity of the tubulus system. As a result, albumin is found within the urine (25). According to an alternative hypothesis – the "albumin retrieval hypothesis" – the amount of filtered albumin during physiologic conditions is much larger than the abovementioned amounts. Following this hypothesis, the tubulus system is highly effective to retrieve intact albumin from the luminal side back to the circulation and remaining albumin is undergoing degradation, leaving only small amounts of intact albumin within the urine (2829). However, there are some flaws within this theory and it is therefore not generally accepted (27). In summary, there are a number of possibilities how albuminuria may evolve, but to date no final prove of the definite underlying mechanism exists. However, even if the exact mechanisms are only incompletely understood, the evidence that urinary albumin excretion is a marker of CV disease is strong and straight forward.
Previously it could be demonstrated that in diabetic patients increased urinary albumin excretion is associated with vascular stiffness (2630) and endothelium dependent vascular dilatation (3132), but not with carotid intima media thickness (30). However, while these studies could show an association between urinary albumin excretion and vascular alterations it is not clear whether urinary albumin excretion itself is part of the pathophysiologic process during development of vasculopathy or just a marker of the disease itself. On the one hand, it is possible that increased urinary albumin excretion simply reflects vascular damage which leacks albumin (33). On the other hand, it might also be the case that leakage of albumin into the vessel wall accelerates inflammatory processes which finally lead to atherosclerosis (2433). And finally, it is not clear whether all conditions or diseases, which are associated with an increased CV risk, are equally associated with urinary albumin excretion (or to the same extent).
In the mid-1990s, Pedersen et al. (34) reported of an increased number of RA patients with MA as compared to controls. The authors found a higher number of patients treated with gold or penicillamine in the MA group, suggesting that treatment with these particular anti-rheumatic drugs may enhance the development of MA. However, it is not established whether MA that is caused by particular drugs confers the same CV risk as MA that develops without that particular drugs. Recently Daoussis et al. (36) could demonstrate that MA [using the European Guidelines for the Management of Arterial Hypertension (35)] is highly prevalent in RA patients (in their cohort in 11.9%). The authors found MA to be associated with the presence of hypertension. This seems to be comparable to the general population, even if there is no prove as a control group is lacking. In former decades proteinuria in RA patients was first of all attributed to different forms of glomerulonephritis or – to a lesser extent – to amyloidosis (37). While this may be true for single patients, firm data to support this assumption are lacking. However, studies on autopsies of RA patients in the 1980ies found a high prevalence of nephrosclerosis (38) as well as "internal proliferation" of the arterioles in the absence of hypertension (39). These findings may suggest "vascular damage" in the investigated RA patients. Thus, the presence of increased urinary albumin excretion or overt proteinuria should not solely raise the suspicion of glomerulonephritis or renal amyloidosis but also to the likely presence of (advanced) microvascular injury. As pointed out above, urinary excretion of albumin shifts away from a pure marker of kidney damage and is more and more regarded as a marker of CV risk. Whether in our study RA patients with incipient renal amyloidosis are included remains open. Clinical findings to support this are lacking. However, renal amyloidosis can only be confirmed by renal biopsy, a procedure which would have not been justified in our patients with low levels of proteinuria.
In the present study we have used the 1987 American College of Rheumatology RA criteria for inclusion of RA patients. We expected that urinary albumin excretion will not be substantially altered early in the RA disease course. Thus, whether urinary albumin excretion would also be increased in RA patients if the 2010 American College of Rheumatology/European League Against Rheumatism RA classification criteria would have been used – which will likely lead to the inclusion of RA patients with shorter disease duration – remains open. Going further, we could not examine the association of urinary albumin excretion and AIx with vascular events, as the number of patients with former CV events was too small. The number of patients with diabetes, which is a main driver of urinary albumin excretion, was large enough to allow the examination of the effect of diabetes on ACR. However, a number of other co-morbidities might also be of relevance with regard to albumin excretion and vascular function. The limited number of patients with other specific co-morbidities precluded such further analyses. In the present study we have excluded patients with inflammatory rheumatic disorders other than RA. Therefore, it was not possible to investigate whether non-RA inflammatory disorders, which may have varying atherogenic pathways, will have a different effect on urinary albumin excretion. Comparative studies with other inflammatory rheumatic disorders would be valuable to answer this question (40).
In conclusion, given the present data it appears that urinary albumin excretion in patients with RA or DM or both is higher than in subjects without RA and without DM, thereby representing a higher CV risk in the former group. However, there is substantial overlap between the groups. We did not find any correlation between AIx, a marker of vascular dysfunction, and ACR.

 XML Download
XML Download