

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Suicide is an emerging social problem in many countries, and nearly one million people worldwide die as a result of suicide each year.6) According to the National Statistical Office of South Korea, the number one leading cause of death in young people (15-24 years) is suicide. Korea has the highest prevalence of suicide among Asian countries, with a rate of 26.1 per 100,000 (World Health Organization, 2008). People use a variety of methods to commit suicide, including self-poisoning, cutting, hanging, falling, gunshot injury, asphyxia, and traffic-related injury.1)
Among these methods, jumping from a high place is frequently used due to availability and the severe bodily damage inflicted by falling.5) Fracture of spine and skeleton and injury to the head and internal organs are some of the injuries that can be inflicted by suicide jumps.5) In this study, we investigated eight patients diagnosed with vertebral burst fracture after a suicide attempt. The aim of this study was to review patients who were admitted to the department of neurosurgery at author's hospital for treatment of vertebral burst fractures due to attempted suicide and to analyze patient characteristics, therapeutic modalities, and compare these injuries with non-suicide related falls and evaluate the initial assessments of these patients.
Materials and Methods
This was a retrospective study of patients who were diagnosed with vertebral burst fractures after attempted suicide. Total 1, 148 patients who had traumatic spinal injuries were admitted to the department of neurosurgery of a single center between 2003 and 2012. Among these patients, eight patients (0.7%) were suicidal jumper. The data were obtained from the clinical charts of patients and through interviews at an outpatient clinic. Demographic data such as age, gender, underlying medical disease, and previous suicide attempts were recorded. We also collected imaging data including X-ray, computed tomography, and initial emergency department magnetic resonance imagings, as well as preoperative and postoperative imaging.
Results
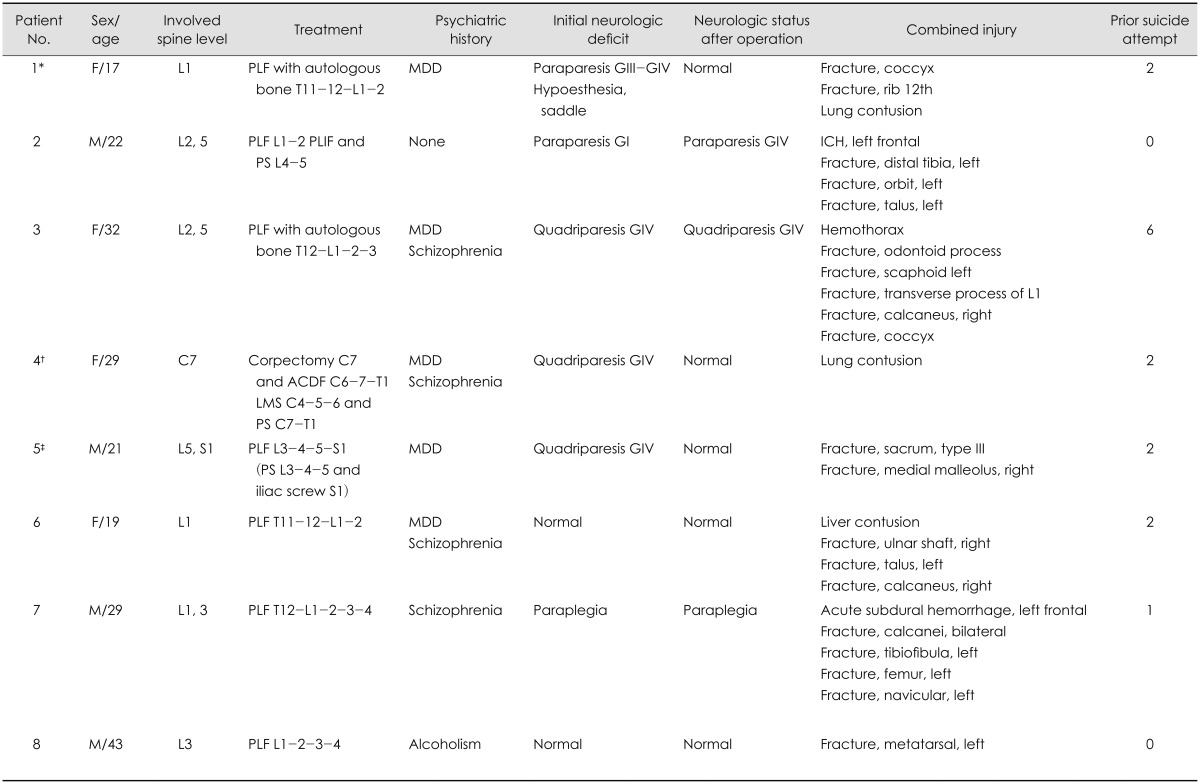
A total of eight patients were reviewed. The mean age of the patients was 26.5 years and four women and four men were included. There were eleven vertebral burst fractures among eight patients. Of the fractures, five fractures were at the thoracolumbar junction, five fractures were in the lumbosacral area, and one fracture was a cervical lesion (Table 1).
Five patients had major depressive disorder which was the most common disease, four patients had schizophrenia and three patients had both and one other patient did not have any psychiatric history. Five patients had made previous suicidal attempt by cutting or drug abuse, and the number of previous attempts ranged from one to five.
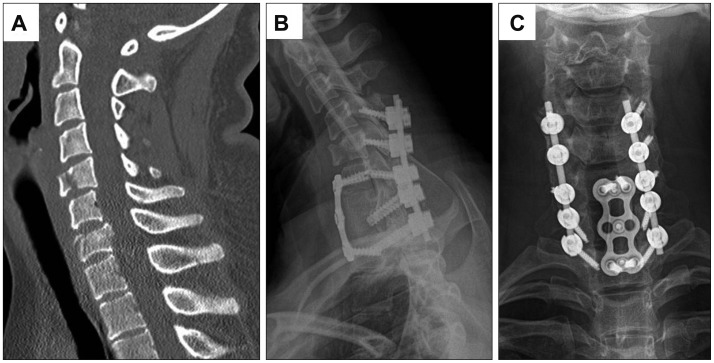
All patients were underwent fusion operations via posterior approach with or without autologous bone for repair of vertebral burst fractures (Figure 1). The patient with a burst fracture of the seventh cervical vertebrae underwent both anterior and posterior fusion (Figure 2).
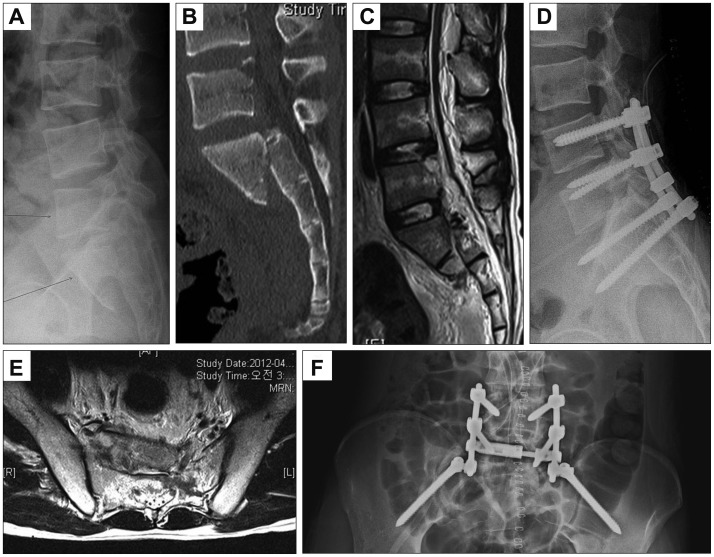
There were various combined injuries in addition to the vertebral burst fractures. Five patients had fractures on foot such as fracture of talus, navicular, calcaneus or metatarsal bones and three patients had fractures of ankle. Five patients had ankle or foot fractures, and four patients underwent surgery for their ankle or foot injuries in the orthopedic department. One patient was diagnosed with a type 3 sacral fracture (Figure 3) and one patient had an acute subdural hematoma and underwent emergency surgery. Injury to the internal organs, such as lung or liver contusion, was diagnosed in three patients. Patients also were suffered various fractures at other locations, including the ribs, odontoid process, transverse process, ulna, scaphoid, and coccyx, according to the impacted site.
Six patients showed impaired neurologic function immediately after trauma, and five patients showed improved or unchanged neurologic status after operation. One patient showed complete cord injury and did not recover in spite of emergency operation.
All patients were transferred to the department of psychiatry after finishing neurosurgical management. The department of rehabilitation also participated in initial therapeutic plans for early rehabilitation.
Discussion
Jumping is the most common method used by those who commit suicide, especially by those in urban societies, and previous studies have shown that this method for attempting suicide can result in various types of injuries to all areas of the body.1,5) We reviewed eight patients who were diagnosed with vertebral burst fractures after attempted suicide by jumping.
The mean age of the patients reviewed in this paper was 26.5 years old, which is much younger than the average age of patients diagnosed with vertebral burst fractures that are a result of accidental falls. This is likely because attempting suicide is more common among younger age groups. Likewise, the leading cause of death for people in their 20s and 30s in South Korea is suicide.
Most of the patients in this study had prior psychological problems and had attempted suicide several times previously such as cutting or drug abuse. Five patients had major depressive disorder which was the most common disease, four patients had schizophrenia and three patients had both. Suicidal ideation is highly prevalent (58%) in patients with major depressive disorder, and suicide is the primary cause of mortality (20.4%) in depression.9) One study has suggested that major depressive disorder will be the second-highest cause of global morbidity and mortality by 2020.6) Generally, between 20% and 65% of patients with major depressive disorder had a history of attempted suicide.7) There is one case of a patient who tried to commit suicide due to alcohol induced delirium tremens. According to one report, up to 24% of male and 17% of female suicide decedents were intoxicated with alcohol at the time of death.4)
In this study, lumbar injury showed more than cervical injury in patients attempting suicide. The most common affected site was L1, followed by L2 and L3. Vertebral burst fractures of the thoracolumbar junction, which is the most vulnerable area for spinal injury, may be caused either by direct impact or by the axial loading seen in feet-first landings.3) This reason for the vulnerability of the thoracolumbar junction is that it is the converting zone from the thoracic kyphosis to the lumbar lordosis, the junction between fixed and mobile segments, and the junction between the thoracic vertebrae, at which the ribs are articulated, and the lumbar vertebrae, at which the ribs are not articulated.2) There were also burst fractures of the cervical and sacral area, which may be due to more powerful impacts to this area. Interestingly, Teh et al.10) reported that more cervical spine injuries were seen in patients who had suffered accidental falls than in people attempting suicide by jumping. However, Richter et al.8) found no significant difference in the number of cervical spine fractures between people attempting suicide by jumping and those injured in accidental falls. In comparing the patterns of injuries after suicidal and accidental falls there is a slightly higher incidence of spinal injuries after suicidal jumps. Fractures of the lumbar spine seem to be more frequent in suicidal jumpers.8) Moreover, because people attempting suicide by jumping typically fall from greater heights than those who fall accidentally, their vertebral burst fractures tend to be more severe and they show a higher mortality rate than patients fell accidentally. Although Richter et al.8) reported that no significant difference in the pattern of injury between deliberate and accidental falls was found, there was a higher incidence of isolated injuries in all patients after unsuccessful suicidal jumps.
All patients were underwent operations for repair of vertebral burst fractures. The performed operative technique was not different from that used to treat burst fractured due to accidental falling. There are various methods to manage vertebral burst fractures, including bracing and operation.2) For cases requiring surgery, there are many surgical techniques available, but it is widely accepted that the goal of surgery for thoracolumbar burst fractures is decompression of the neural elements, correction of spinal deformities, and fusion with stabilization.3) For performing early rehabilitation, surgical treatment should be considered than conservative care.
There were several combined injuries in the patients reviewed here, especially in the lower limbs. Five patients had fractures on foot such as fracture of talus, naviculus, calcaneus or metatarsal bones and three patients had fractures of ankle. Calcaneus fracture due to landing feet-first was the most common (Figure 4). Many previous studies have found that fractures of the lower limbs, including the calcaneus and other ankle bones and the shafts of long bones are all more common in intentional falls.5,10) Because people jumped for the purpose of suicide do take a defensive posture when jumping, they tend to land feet first, whereas patients injured in accidental falls typically show injury to other parts of their bodies. Calcaneus fracture is combined with thoracic or lumbar spine fracture in 75% of fall patients, regardless of intention.10) Therefore, whole spine imaging can be considered if the patient has calcaneal fracture after fall down in the suicidal jumping patients.
Conclusion
Suicidal jumper is different from incidental faller in some aspects because of different injury mechanism. So, understanding these differences is important for the assessment and management of these patients. For managing suicidal jumper, physician had to consider patients' age, affected site, psychiatric problem and combined injuries.


 XML Download
XML Download