

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The standard of national health was significantly improved as Korea achieved economic development and enhanced dietary life by developing into a modern industrial society. Furthermore, with improved health environment, better medical service and higher interest on public health, the average lifespan of Korea has increased along with the elderly population ratio. Hereupon, different disease characteristics are being presented due to the increase in adult diseases (or lifestyle diseases), such as cancer, hypertension and diabetes. The main causes of adult diseases are reported as the following: dietary life, genetic factors, lack of exercise, stress, and environmental pollution. Among these causes, dietary habit is viewed as the factor that is easiest to control [1]. Effective countermeasures for adult diseases can induce proper dietary habit from the aspect of preventive medicine, and can also reduce the increasing medical costs spent in treating adult diseases [2]. Recently, Korea is also focusing on health functional foods (HFFs) that emphasize the tertiary function of food, thus physiological regulation, rather than its primary and secondary functions, thus life maintenance and selection of favorite foods [3]. The HFF market is rapidly expanding not only in Korea but worldwide, in step with the expectations of consumers that hope to achieve greater effects within a short period of time by consuming non-medical food products rich in active components with functional characteristics. The size of the HFF market in Korea was estimated to reach 3 trillion KRW in 2009 and is continuously achieving more than 10% growth each year [4].
HFFs, which are rapidly increasing in consumption both domestically and abroad, can contribute to the maintenance and enhancement of public health when consumed appropriately. However, if the products are misused or abused due to excessive propaganda or inappropriate labeling, it may harm the health of people or prevent the acquisition of positive effects [5]. Hereupon, since the enactment of the law for HFFs on August 26, 2003, the HFF management system has been implemented through the enactment and announcement of enforcement ordinance and the promulgation of subordinate provisions for law execution, such as enforcement regulations and related laws. The law for HFFs aims to contribute to the improvement of national health by enhancing the production and quality of safe HFFs, promotes the establishment of proper distribution and sale order for protecting consumers and attempts to increase competitiveness by supporting and fostering the industry [6]. By enacting the law for HFFs, consumers can easily acquire accurate information on the products they wish to purchase, reduce distrust for HFFs and prevent the harm of purchasing HFFs by mistaking them for medical products.
Many studies have been carried out and are still being conducted to increase the positive effect of HFFs and reduce the harmful effect generated through incorrect intake [7-9]. Although several researchers have investigated the intake of HFFs in Busan and Gyeongnam area [10,11], insufficient research was carried out on the factor analysis related with the intake of HFFs. Hereupon, in addition to the intake of HFFs among adults living in Busan and Gyeongnam area, this study surveyed the demographic characteristics, dietary habits, health habits and the knowledge level of subjects in order to conduct a comparative analysis on these factors according to the intake of health functional foods.
Materials and Methods
Subjects
The study population consisted of men and women in their 20s-50s living in Busan and Gyeongnam area. The questionnaires were self-recorded by the subjects. A total of 680 questionnaires were distributed and 650 questionnaires were collected (collect rate 95.6%). A total of 634 questionnaires (male: 305, female: 329) were used for this study after the questionnaires that lacked answers or were judged inappropriate according to subject selection standards have been excluded.
Survey content and method
By reviewing various data included in precedent studies that were carried out on adults, items corresponding to the purpose of this study were selected, modified, complemented and written for the questionnaire. The items were related with the sociodemographic characteristics, health habits, dietary habits, intake of HFFs, factors influencing intake, perception and knowledge of HFFs of subjects.
To observe the sociodemographic characteristics of the subjects, the items were composed of gender, age, marital status, educational level, occupation and average monthly income.
To observe the living habits related with the health of the subjects, the items were composed of BMI classification, personal opinion on one's body shape, health condition, disease, type of disease, number of health examinations received, smoking, drinking, exercise and health management method.
To observe the dietary habits of the subjects, the items were composed of meal time, appetite, number of meals, dietary attitude, eating breakfast, degree of food seasoning and amount of drinking water per day. For the dietary attitude, 11 items asking about the frequency of food intake was scored on a range of 0-4 points and the points were added up to classify the dietary attitude of research subjects into excellent, good, average, poor and very poor.
To observe the intake condition of HFFs, this study investigated the types of HFFs and the experience of consuming the different food types. In order to research the extensive intake tendency of subjects, the items were composed of 37 types of generic HFFs (including dietary supplements) acknowledged by the law for HFFs [12] as well as 33 food types widely consumed for health although not acknowledged by the relevant law. Research subjects were instructed to select HFFs that they were currently consuming or had consumed during the past year. Subjects were allowed to select multiple answers. Furthermore, this study surveyed the reason for ingesting HFFs, motive of intake, place of purchase, purchaser, intake period, average expense and preferred form. In the factor analysis related with the intake of HFFs, this study only analyzed the intake of generic HFFs to increase the validity of research.
To observe the perception and knowledge of HFFs, this study investigated 5 items regarding the definition of HFFs, method for acquiring knowledge and the concept and classification of other terms related with HFFs.
Statistical analysis
All of the collected data were analyzed using SPSS/WIN Program (Ver.12.0). Statistical methods such as frequency analysis, crosstabulation, mean, standard deviation and student t-test were used according to the research problem. Logistic regression was used to analyze factors that influence the intake of HFFs. Two-sided p values less than 0.05 were considered statistically significant.
Results and Discussion
Sociodemographic characteristics of research subjects
This study included a total of 634 subjects. 305 (48.1%) were 'men' and 329 (53.6%) were 'women'. 230 (36.3%) were in their '20s', whereas 203 (32%) were in their '30s', 102 (16.1%) were in their 50s and 99 (15.6%) were in their '40s'. For marital status, 362 (57.1%) were 'married', 268 (42.3%) were 'single' and 4 (0.6%) subjects responded 'other', thus presenting a larger number of married subjects. For educational level, 307 (48.4%) were 'college graduates', 275 (43.3%) were 'high school graduates', 25 (3.9%) were 'graduate school graduates or of higher education', 23 (3.6%) were 'middle school graduates' and 4 (0.6%) were 'elementary school graduates', thus presenting a high level of education in general. For occupation, 175 (27.6%) were 'professionals', 140 (22.1%) were 'students' and 86 (13.6%) were 'technicians'. Statistics presented a high ratio of professionals and students and similar results were presented according to gender. For the average monthly income, 203 (32.0%) earned 'less than 1 million KRW', 190 (30.0%) earned '1-2 million KRW' and 157 (24.8%) earned '2-3 million KRW'. The reason why many subjects answered 'less than 1 million KRW' is stipulated to be related with the high ratio of subjects in their 20s (Table 1).
Intake of HFFs
To observe the intake condition of research subjects, this study investigated generic HFFs acknowledged by the law for HFFs and other health foods that are frequently ingested for health although not acknowledged by the relevant law (Table 2). Among research subjects, 269 (42.4%) had experience of ingesting generic health functional goods in the past year, whereas 229 (36.1%) did not have the relevant experience. 137 (21.6%) subjects consumed food products not acknowledged as HFFs, such as special nutritious foods, medicinal herbs and oriental medicine, self-preservation food and folk medicine. The total intake rate of HFFs and other health food products was presented as 64.0%, which is lower than the results shown in the research conducted by Shin [13] (68.8%) and the research conducted by Nam [14] (66.7%) and similar to the research conducted by Yoon [15] (61.2%). The intake rate was analyzed as low when observing the fact that diverse products were selected in this study. Only 108 men (35.4%) ingested HFFs, thus presenting a large difference from 161 women (48.9%) that ingested HFFs. 68 men (22.3%) and 69 women (21.0%) answered that they had ingested other health food products.
Next, this study observed the intake of HFFs and other health food products according to food groups (Table 2). Currently, the 'dietary supplement food' and 'health functional food' are the generic HFFs acknowledged by the law for HFFs. 312 (76.8%) subjects ingested 'dietary supplement foods', 263 (64.8%) ingested 'fruit or vegetable juice', 260 (64.0%) ingested 'HFFs', 120 (29.6%) ingested 'medicinal herbs and oriental medicine' and 101 (24.9%) consumed 'self-preservation food and folk medicine'. The study conducted by Choi [16], who surveyed the intake of generic food products, also presented similar results with this study as 'dietary supplement foods' accounted for the highest ratio. This study also presented high ratio of food products not acknowledged as HFFs, such as 'fruit or vegetable juice', 'medicinal herbs and oriental medicine' and 'self-preservation food and folk medicine', thus indicating the need to manage other health food products according to a national system. Currently, many food products are expected to join the ranks of HFFs due to the deregulation of the HFF law, which in turn implies the need to establish a system for controlling the HFF market. Among men, 113 (64.2%) ingested 'fruit or vegetable juice', 115 (65.3%) ingested 'dietary supplement foods', 100 (56.8%) ingested 'HFFs' and 57 (32.4%) ingested 'medicinal herbs and oriental medicine' and 'self-preservation food and folk medicine'. Among women, 198 (85.7%) ingested 'dietary supplement foods', 160 (69.6%) ingested 'HFFs', 150 (65.2%) ingested 'fruit or vegetable juice' and 63 (27.4%) ingested 'medicinal herbs and oriental medicine'. When compared with women, men presented a higher intake ratio of 'self-preservation food and folk medicine'. On the other hand, women presented a higher intake ratio of 'dietary supplement foods', 'grain and bean products' and 'fermented food'.
Information related with the intake of HFFs
Table 3 presents the information related with the intake of HFFs by the subjects. The most common reason for ingesting HFF was 'maintenance and enhancement of health' (36.8%), followed by 'fatigue recovery' (20.4%) and 'nutrition supply' (17.1%). Women placed a greater emphasis on 'prevention and treatment of disease' and 'beauty treatment' whereas men focused more on 'maintenance and enhancement of health' and 'fatigue recovery'. These results were statistically significant (p < 0.01). The most common motive for ingesting HFFs was 'self-judgment' (44.6%), followed by 'recommendation of neighbors and friends' (39.8%). 'Self-judgment' was selected by 49.1% of men and 41.6% of women, whereas 'recommendation of neighbors and friends' was selected by 42.2% of women and 36.1% of men. This shows that when compared with men, women take a more subjective approach to the intake of HFFs. These results were also statistically significant (p < 0.05). The most common route for purchasing HFFs was the 'HFFstore' (36.9%), followed by 'pharmacy' (24.5%) and 'door-to-door sales' (14.1%). 'Home shopping' and 'department store, discount store' presented high response rate among men, whereas 'door-to-door sales' was popular among women. These results were statistically significant (p < 0.001). The results of this study were also similar to studies conducted by Yoon [11] and Shin [13], which presented high response rates for 'pharmacy' and 'HFF store'. 45.7% of subjects 'personally' purchased the HFFs whereas 33.1% purchased through 'family (siblings or parents)' and 16.7% purchased through their 'spouse'. 53.4% of women purchased the products 'personally', which is a ratio that far exceeds that of men, who presented a high ratio of purchasing products through their 'spouse' (28.7%). These results were statistically significant (p < 0.001). The intake period of HFFs was surveyed as '1-2 months' (45.7%), followed by '3-6 months' (28.3%) and '7-12 months' (11.2%), thus presenting a high ratio of short-term intake. Women presented a slightly higher ratio of long-term intake than men, but the result was not significant. For the number of HFFs simultaneously ingested, 50.9% of subjects ingested '1 type' of health functional food, 26.8% ingested '2 types' whereas 10.8% ingested '3 types'. Similar results were also presented according to gender. Women presented a slightly higher ratio than men in the intake of '5 types or more', but the result was not significant. The average expenditure for HFFwas presented as '10,000-50,000 KRW' (55.4%), followed by '60,000-100,000 KRW' (23.0%). Women generally presented a higher level of average expenditure than men, but the result was not significant. 'Below 50,000 KRW' also accounted for the highest ratio in the studies conducted by Yoon [11] and Kim [17]. Next, the preferred form of HFF was presented in the order of 'capsule' (42.8%), 'liquid' (24.5%) and 'refined substance' (16.3%). Men presented a tendency to prefer the 'liquid' form more than women, who in turn preferred 'capsule' and 'refined substance' more than men. However, the results were not significant. 71.0% of subjects presented 'average' satisfaction for the expected effects of HFFs, whereas 18.2% were 'satisfied' and 9.7% were 'dissatisfied'. Both men and women presented average satisfaction for the expected effects of HFFs while viewing the product cost to be expensive. 61.7% of subjects responded that there were 'no side effects' related with the HFFs, whereas 28.6% were 'unsure' and 9.7% answered that 'side effects' did exist. The results gained from the studies conducted by Yoon [11] and Kim [17] were similar to this study in that 11.2% and 13.3% of subjects responded that side effects existed, respectively. However, the study conducted by Kang [18] presented difference from this study as the side effect rate was shown as 20.3%, 24.8%. The most common symptoms experienced in relation to the side effects of HFFs were 'stomachache and stomach disorder' (53.8%), followed by 'skin trouble' (23.1%). Women presented a higher ratio of 'stomachache and stomach disorder' than men, but the result was not statistically significant.
Factors related with intake of HFFs
In the factor analysis related with the intake of HFFs, this study analyzed the intake of generic HFFs to increase the validity of research (Table 4). Among various sociodemographic characteristics according to the intake of health functional food, age, marital status, educational level, occupation and average monthly income did not present statistical significance. However, 161 (61.9%) women had experience of ingesting HFFs, thus exceeding the ratio of 108 men (45.6%) that had intake experience. This result was statistically significant (p < 0.001). The study conducted by Nam [14] presented similar results with this study as significant difference was presented in the intake of HFFs according to gender. However, the study conducted by Um [19] presented different results with this study as the intake rate was increased with higher age and average monthly income.
Among the various health habits analyzed according to the intake of HFFs, BMI, personal opinion on one's weight, health condition, number of health examinations received and exercise presented statistical insignificance, whereas disease, smoking and drinking presented statistically significant results (Table 5)(p < 0.05). HFF intake rate was higher among subjects with disease. Also, higher intake rate was shown among non-drinkers and non-smokers. Significant results were not presented between men and women when the intake of HFFs, smoking and drinking were analyzed according to gender, thus implying that the significance presented according to the intake of HFFs, smoking and drinking was caused by gender differences. The study conducted by Nam [14] also presented high HFF intake rate among non-smokers and non-drinkers, whereas the study conducted by Um [19] presented results similar to this study by verifying that the intake rate was higher among subjects with chronic diseases.
Logistic regression analysis was carried out to investigate the factors that influence the intake of HFFs. Results are as shown in Table 6. This study only analyzed the intake of generic HFFs to increase the validity of research. By analyzing all items related with sociodemographic characteristics, health habits and dietary habits and the intake of HFFs, results showed that the intake rate of HFFs was increased by 1.891 times in women when compared with men. Also, the intake rate was increased by 1.478 times among subjects that ate bland food when compared with those enjoying salty food. The results were statistically significant (p < 0.05).
Perception and knowledge of HFFs
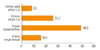
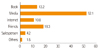
For the survey item 'Have you heard of the definition of HFFs?' selected to investigate the perception of HFFs, 49.2% of subjects answered 'Yes, I have heard of it', followed by 'I know the definition' (26.2%), 'I have neither heard nor know the definition' (16.1%) and 'I am well aware of it' (8.5%), thus showing that many people know or have heard of HFFs (Figure 1). For the survey item on the method for gaining information on HFFs, 52.1% replied that they gain information through 'media', followed by 'friends or acquaintances' (18.3%), 'books' (13.2%) and the 'internet' (10.8%), thus presenting that much information was gained through 'mass media', such as TV and radio. In this regard, providing accurate, simple information through media can be viewed as an important advertising method for HFFs (Figure 2). The study conducted by Nam [14] et al. indicated that the routes for gaining information regarding HFFs included 'books' (28%), 'acquaintances' (26%) and 'media' (15%), in the respective order, thus presenting differences from this study. However, the study conducted by Yoon [15] presented similar results with this study by reporting that subjects gained information on HFFs through 'media' (32.9%), 'word-of-mouth' (31.6%), 'hospital and pharmacy' (13.3%) and 'HFFstores' (9.7%). If it is easier to process information related with HFFs, the consumer ability to properly judge HFFs is improved [20] and the consumers' health knowledge and attitude are enhanced to increase the market share of HFFs [21]. In this regard, it is important to provide channels through which consumers can gain information on HFFs more easily and quickly.
Next, Table 7 presents the responses for the 5 items selected to investigate the consumers' knowledge of HFFs. For the survey item 'HFFs and health supplement foods are the same', 159 men (52.1%) answered 'false', 83 men (27.2%) answered 'not sure' and 63 men (20.7%) answered 'true'. Among women, 172 (52.3%) answered 'false', 109 (33.1%) answered 'true' and 48 (14.6%) answered 'not sure'. The response rate of women was higher than that of men and presented statistical significance (p < 0.001). For the survey item 'All products commonly advertised to be good for health are HFFs', 189 men (62.0%) answered 'true', 66 (21.6%) answered 'not sure' and 50 (16.4%) answered 'false'. Among women, 250 (76.0%) answered 'true', 52 (15.8%) answered 'false' and 27 (8.2%) answered 'not sure'. Women also presented a higher response rate for this item and men showed a high response rate for 'not sure'. Results were statistically significant (p < 0.001). For the survey item 'HFFs have medical effect and can thus treat diseases', 203 men (66.6%) answered 'true', 73 (23.9%) answered 'not sure' and 29 (9.5%) answered 'false'. Among women, 239 (72.6%) answered 'true' and 45 (13.7%) answered 'false' and 'not sure', respectively. Results presented significance according to gender (p < 0.01). For the survey item 'HFFs can be expressed to be effective in preventing or treating certain diseases', 113 men (37.0%) answered 'not sure', 100 (32.8%) answered 'true' and 92 (30.2%) answered 'false'. Among women, 129 (39.2%) answered 'true', 113 (34.3%) answered 'false' and 87 (26.4%) answered 'not sure'. Results presented significance according to gender (p < 0.05). According to the survey item for selecting HFFs among 7 types of products, the mean and standard deviation of men and women were presented as 0.59 ± 1.19 and 0.67 ± 1.17, respectively, with 1 being the top score. Women presented a higher score than men and the result was statistically significant (p < 0.001). Women presented a higher response rate than men in all items and the result was statistically significant. This implies that women have more knowledge of HFFs than men in general. Furthermore, as the response rate for survey items 'All products commonly advertised to be good for health are HFFs' and 'HFFs have medical effect and can thus treat diseases' was relatively higher than other items, it can be known that survey subjects do not have blind faith regarding the effect of HFFs. In relation to the items above, this study observed the relationship between the knowledge and intake of HFFs. For the survey item 'HFFs can be expressed to be effective in preventing or treating certain diseases' and the item questioning the intake of HFFs, higher score and response rate were presented by subjects that had experience ingesting HFFs and statistically significant results were gained (p < 0.05, p < 0.01). However, significant results were not gained between the intake experience and knowledge level for the remaining items. The study conducted by Park [22] presented similar results with this study as significant relations were not presented between the knowledge level and intake of HFFs.
Conclusion
In conclusion, by surveying sociodemographic characteristics, dietary habits and health habits related with HFFs, it was shown that the intake of HFFs was presented differently according to gender, smoking, drinking and disease of individuals. In particular, the HFF intake rate presented the most significant difference according to gender. Among the factors related with the intake of HFFs, significant difference was shown between men and women in the reason for ingesting HFFs, motive of intake and purchaser. Thus, it was verified that gender was a factor that significantly influences the intake of HFFs. In this regard, it is important to develop HFF educational programs in consideration of the different characteristics shown according to gender and to provide an educational program in which subjects can manage their health by selecting health functional foods appropriate for their dietary and living habits.







 XML Download
XML Download