

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Treatment options for cerebral arteriovenous malformations (AVMs) have evolved rapidly over the past two decades, although the optimal management paradigm remains controversial.35) Advances in microsurgical techniques and equipment, technologies for endovascular embolization, and stereotactic radiosurgery (SRS) have resulted in a number of safe and effective treatments, but selecting an appropriate treatment strategy remains challenging in many cases.1)2)3)4)5)12)13)14)15)16)17)18)19)20)21)22)23)24)25)26)27)28)29)30)36)37)39)40)41)49)50)51)52)54)57) Of the various interventional options for AVMs, surgical resection remains the gold standard.11)33)34)48)
Preoperative embolization is a valuable neo-adjuvant treatment that has been shown to be effective in decreasing operative time, blood loss, and morbidity and mortality.10) The majority of modern AVM embolization is performed using ethylene vinyl alcohol copolymer (Onyx; ev3 Neurovascular, Irvine, California, USA).43) However, at our institution, we have found that more traditional embolic agents, such as silk suture and polyvinyl alcohol (PVA) particles, offer unique advantages over Onyx for preoperative devascularization of appropriately selected nidi.
The aims of this retrospective cohort study are to (1) describe our technique for silk suture and PVA particle embolization (SPE) of cerebral AVMs and (2) analyze the post-embolization and postoperative angiographic and clinical outcomes in a modern, single-center series.
MATERIALS AND METHODS
Patients selection and study design
We performed a retrospective review of all patients who underwent preoperative embolization of cerebral AVMs at the University of Virginia between January 2000 and June 2013. Inclusion criteria for the study were (1) preoperative SPE of the AVM nidus, (2) AVM surgical resection performed at our institution, (3) sufficient data to ascertain baseline patient demographics, nidus angioarchitecture, and post-treatment clinical and angiographic outcomes. Exclusion criteria were (1) patients with vascular malformations other than AVMs, (2) nidi primarily embolized with agents other than silk suture and PVA particles, and (3) AVMs surgically resected at other institutions. Concomitant use of embolic agents other than silk suture of PVA particles, such as detachable coils, was noted. Inpatient and outpatient medical charts and imaging were reviewed for patient and AVM characteristics, pathologic details, intraoperative findings, complications, and outcomes. This study was approved by the University of Virginia institutional review board (IRB).
Embolization procedure
Selection of AVMs for pre-operative SPE was made on an individualized basis after a discussion between the neurosurgeon and neurointerventionalist regarding the nidus angioarchitecture. All cases were performed using high-resolution biplane digital subtraction angiography under general anesthesia. Access to the femoral artery was obtained in standard fashion. Intravenous heparin was intermittently administered throughout the procedure to achieve an activated clotting time (ACT) of between 250-300 seconds. The heparin was not reversed following the procedure.
A diagnostic angiogram of the bilateral internal and external carotid arteries and vertebral arteries was performed in order to define the nidus angioarchitecture, including feeding arteries, draining veins, presence of arterial or venous aneurysms, intranidal arteriovenous shunts, and/or venous strictures. After determining the most appropriate arterial branch for embolization, a microcatheter, most commonly an Echelon 10 (ev3 Neurovascular, Plymouth, MN, USA), was advanced into the target pedicle under roadmap guidance, and embolization was performed. Multiple cut portions of silk suture threads, approximately 0.5 mm in length, and PVA particles were deployed into the pedicle via the microcatheter until adequate devascularization of the targeted portion of the nidus was achieved, as deemed by the treating neurointerventionalist. Generally, the silk suture was deployed first followed by PVA particles. Control angiograms were intermittently performed after SPE of each arterial branch to assess the degree of nidal devascularization. Deployment of other embolic agents, such as Gelfoam (Pfizer, New York, NY, USA) or coils, was performed, as necessary, after initial SPE in order to improve nidus devascularization and/or to prevent reflux of the silk suture and particles. A final control angiogram was performed after the embolization procedure to assess the residual nidus.
Baseline variables and treatment outcomes
Patient variables were gender, age, clinical presentation, and medical comorbidities. AVM variables were location, venous drainage pattern, maximum nidus diameter, nidus volume, Spetzler-Martin grade, and presence of associated arterial and venous aneurysms.48) Maximum nidus diameter was measured on pre-embolization angiography. AVMs were assumed to be ellipsoid and the volume was calculated accordingly. The embolization variable was the embolic agent used. Surgical variables were amount of intraoperative blood loss and duration of procedure.
Treatment outcomes were stratified by post-embolization and post-surgical outcomes. Post-embolization outcomes were degree of AVM nidus obliteration, modified Rankin Scale (mRS) after embolization (prior to surgery), and procedural complications. Post-embolization angiograms were assessed for the volume of residual nidus compared to the pre-embolization angiogram. The degree of AVM obliteration was categorized as < 25%, 25-50%, 50-75%, and > 75%. Post-surgical outcomes were degree of AVM nidus obliteration (based on postoperative angiography), postoperative complications, and mRS at the most recent clinical follow-up. All imaging studies were reviewed by a neurosurgeon and neuroradiologist at our institution. Categorical variables were reported as a frequency, and continuous variables were reported as a median and range.
RESULTS
Study population and clinical presentation
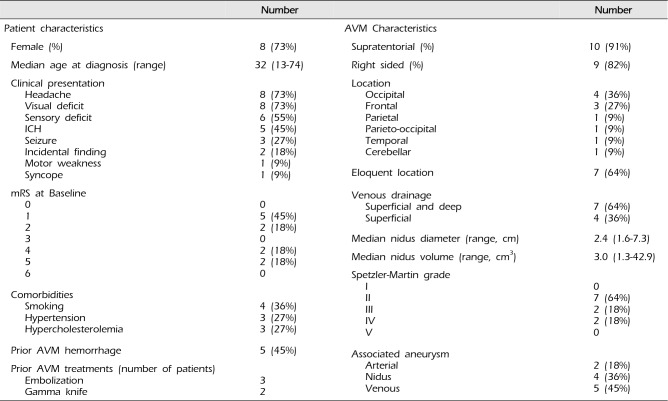
A total of 17 AVM patients underwent 24 SPE procedures during the study period. Six patients (12 SPE procedures) were excluded for subsequent treatment with SRS (four patients) or undergoing surgery at another institution (two patients). This yielded 11 patients who underwent 12 preoperative SPE procedures for analysis. The patient and AVM characteristics are summarized in Table 1. Eight patients were female (73%). The median age of all patients was 32 years (range 13 to 74 years) at the time of initial SPE. The most frequent clinical symptoms at presentation were headache and visual deficit, each in eight patients (72%), sensory deficit in six patients (55%), intracranial hemorrhage (ICH) in five patients (45%; two cases each of intracerebral and intraventricular hemorrhage, one case of subarachnoid hemorrhage), and seizure in three patients (27%). Medical comorbidities included smoking in four patients (36%) and hypertension and hypercholesterolemia each in 3 patients (27%). The mRS scores at presentation were 2 or lower in seven patients (64%) and 3 or greater in four patients (36%). Three patients (27%) underwent prior embolization treatment with material other than silk and PVA particles, and two patients (18%) underwent prior Gamma Knife SRS.
AVM Characteristics
AVMs were supratentorial in 10 cases (91%). They were localized to the right side in nine cases (82%), to the left side in one case (9%), and in the midline in one case (9%). The most common AVM locations were occipital in four cases (36%) and frontal in three cases (27%). Seven nidi were located in eloquent areas (64%), and seven nidi had a component of deep venous drainage (64%). The Spetzler-Martin grade was II in seven patients (64%) and III and IV each in two patients (18%). AVMs were associated with arterial and venous aneurysms in six (55%) and five (45%) cases, respectively.
AVM embolization outcomes with silk suture and PVA particles
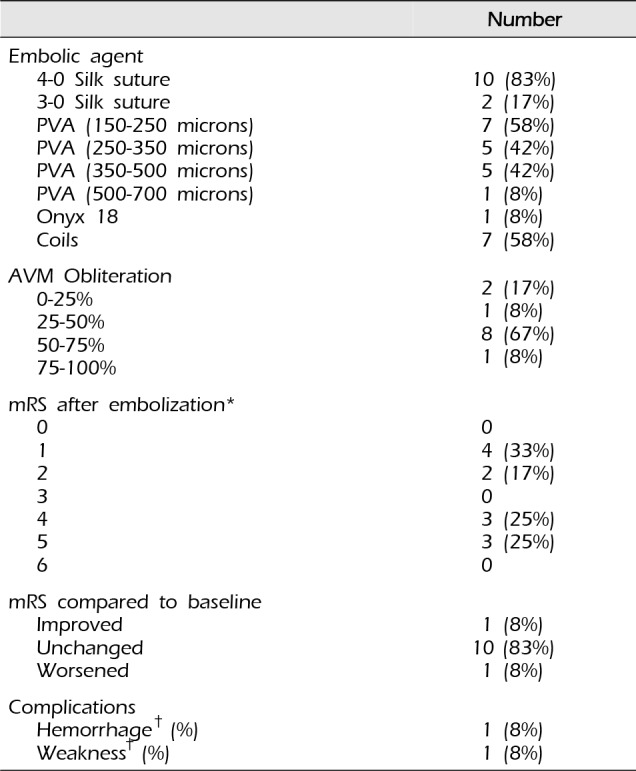
The embolization procedural details and outcomes are summarized in Table 2. In the 12 SPE procedures, the degree of AVM obliteration was < 25% in two cases (17%), 25-50% in one case (8%), 50-75% in eight cases (67%), and > 75% in one case (8%). The arterial pedicle was occluded with coils after SPE in seven cases (58%). Post-embolization complications consisted of ICH, with accompanying hemiparesis, in one patient (8%). There were no cases of post-embolization ischemia, based on clinical or radiologic assessments. Post-embolization mRS was improved in one patient (8%), unchanged in 10 patients (83%), and worsened in one patient (8%).
AVM surgical outcomes
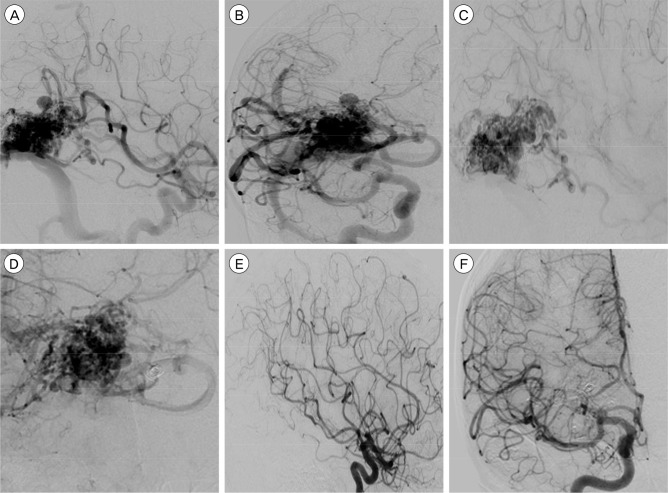
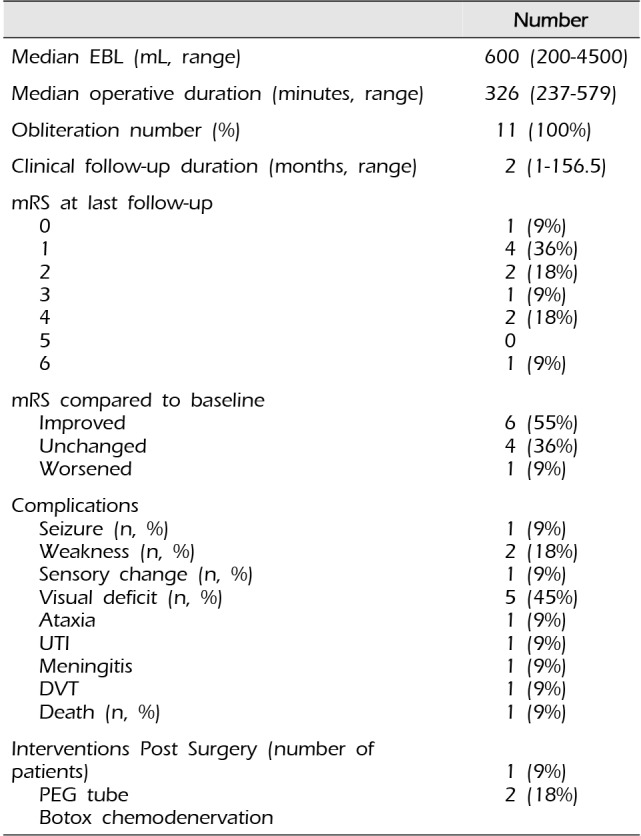
The details and outcomes of the AVM surgical procedures are summarized in Table 3. Of the 11 patients who underwent surgical resection at our institution, at a median interval of one day (range 1 to 3 days) after the most recent SPE embolization, the median estimated intraoperative blood loss was 600 mL (range 200 to 4,500 mL), and the median operative duration was 326 minutes (range 237 to 579 minutes). Based on postoperative angiography (Fig. 1), complete AVM obliteration was achieved in all cases (100%).
At the most recent clinical follow-up (median duration 2 months, range 1 to 156.5 months), the mRS score was 0 in one patient (9%), 1 in four patients (36%), 2 in two patients (18%), 3 in one patient (9%), 4 in two patients (18%), and 6 in one patient (9%). Compared to baseline, six patients (55%) showed improvement from their mRS score, four patients (36%) were unchanged, and one patient (9%) worsened. Postoperative surgical and medical complications included visual deficit in five patients (45%), weakness in two patients (18%), and seizures, sensory changes, ataxia, urinary tract infection, meningitis, deep vein thrombosis, and death each in one patient (9%). Additional interventions performed after AVM resection included botulinum toxin chemodenervation in two patients (18%), and percutaneous endoscopic gastrostomy tube placement in one patient (9%).
DISCUSSION
Preoperative AVM embolization confers a number of potential advantages.6)7) By reducing intraoperative blood loss during AVM surgical resection, preoperative embolization may improve the safety of these procedures by potentially decreasing the technical difficulty of resection and operative duration.10) Embolic agents can be used to mark arterial feeding vessels, which can be difficult to differentiate from arterialized draining veins intraoperatively. Preoperative embolization also devascularizes the deep portions of an AVM nidus, which are difficult to access intraoperatively and are not typically encountered until the later stages of AVM dissection. Premature intraoperative hemorrhage from the deep portion of a nidus can be difficult to control. Thus, preoperative embolization may facilitate AVM circumdissection and extirpation.
In addition to silk suture and PVA particles, cyanoacrylates (e.g. NBCA) and Onyx are two embolic agents used to treat AVMs. NBCA was approved in 2000 after it was shown to be equivalent to PVA for AVM embolization.38) While embolization with NBCA may provide a more thorough and durable nidal devascularization than SPE, NBCA embolization carries a risk of microcatheter tip entrapment within the embolic cast, which can precipitate AVM hemorrhage upon forcible withdrawal of the microcatheter.8)56) Additionally, if NBCA is deployed too rapidly, the target artery may become occluded prior to adequate nidal penetration. Furthermore, the draining vein can become occluded before adequate nidal penetration is achieved and arteriovenous shunting is halted, causing a significant increase in intranidal pressure, thereby incurring a much higher risk of rupture.
Onyx is a permanent liquid embolic agent that is dissolved in dimethyl sulfoxide (DMSO). Once DMSO diffuses into the blood, Onyx precipitates and leads to vascular occlusion.53) Although Onyx may provide superior AVM devascularization compared to either NBCA or silk suture and PVA particles, its risks should be noted. There have been reports linking DMSO to vessel necrosis and neuronal swelling.44) Similar to NBCA, there is also an unavoidable risk of microcatheter entrapment with Onyx embolization, although new microcatheters with detachable tips may lessen the concern for this complication.32)55) Finally, although AVM embolization with NBCA and Onyx can be curative, there remains a small risk of recurrence even after complete angiographic obliteration. Since no single embolic agent, or combination of agents, has been accepted as a clear favorite for AVM devascularization, the nature of each individual nidus and the goals of embolization should be considered when determining the embolic agent of choice for a particular case. Future developments in endovascular technology may further improve the safety of modern embolic agents.
In this study, we report the detailed outcomes of 11 AVM patients who underwent 12 preoperative SPE procedures. The proportion of patients who presented with AVM rupture was 45%, which is slightly higher than prior silk suture embolization series.9)45) One patient, who had a ruptured AVM, experienced post-embolization hemorrhage (8%). In comparison, the rates of AVM hemorrhage after Onyx embolization are as high as 12.5% for ruptured, and 1.6% for unruptured AVMs.32) Although complete AVM occlusion can rarely be achieved with SPE and a significant degree of devascularization may be challenging for SPE of large AVMs, the degree of volume reduction was at least 50% for the majority of SPE procedures (75%). Surgical AVM resection resulted in complete obliteration in all patients (100%), with worsened postoperative mRS in only one patient (9%). Additionally, 64% of patients were functionally independent at a median follow-up duration of two months. Therefore, multimodality AVM management with preoperative SPE and subsequent surgical resection remains a viable combined approach in the modern era.
Reports of AVM embolization with PVA and silk suture are relatively sparse in the literature, due to an overall preference for NBCA and Onyx by many neurointerventionalists. Schmutz et al. reported a series in which silk suture was the main embolic agent in 73 AVM patients, and reported a 1.4% post-embolization hemorrhage rate.45) Histopathological analysis of four patients who underwent silk suture embolization showed an absence or mild amounts of perivascular inflammation and vasculitis.46) In addition to its relatively favorable clinical and histopathological profile, silk suture has a number of definite advantages as an embolic agent.9)47) Silk suture is inexpensive, readily available, easy to manipulate, allows for continuous radiographic monitoring of the microcatheter during and after embolization, and does not interfere with the use of other embolic agents. There is no risk of microcatheter entrapment, as with cyanoacrylates and Onyx.8)32)55) The relatively large cross section of silk suture decreases the risk of inadvertent premature occlusion of a draining vein, although there is limited data to show that the rate of post-embolization AVM hemorrhage is lower with silk suture compared to other embolic agents.
Nidal embolization with PVA particles and silk suture can be performed from a proximally located microcatheter, so that the microcatheter does not have to be positioned within the nidus to proceed with silk suture embolization.9) Therefore, less microguidewire and microcatheter navigation are necessary to perform AVM embolization with PVA particles and silk suture, which may reduce the risk of vascular injury to feeding arteries. However, we avoided embolization of arterial pedicles with an en passage branch or terminal feeding vessel located distal to the microcatheter tip, in order to avoid inadvertent ischemic complications. Whereas Onyx, cyanoacrylates, and microcoils stiffen an AVM nidus, thereby impairing surgical manipulation, silk suture devascularizes the nidus and marks the feeding arteries without significantly affecting its inherent maneuverability and tactile response.9)42)47) Furthermore, we have not found silk suture embolization to result in significant arachnoid scarring, which can occur to a significant extent with permanent agents such as Onyx. This preserves the dissection plane between the AVM and the normal brain parenchyma, thus facilitating surgical resection. A disadvantage of silk suture is its radiolucency, so one cannot readily track the distribution of silk suture during and after embolization. The use of radiopaque silk sutures with platinum markers has been proposed to overcome this limitation, although its clinical implications have not been thoroughly evaluated.31)
The interpretation of our results is limited, in part, by the study design as a retrospective, single-center cohort study. Thus, our study is subject to the selection biases of the neurointerventionalists and neurosurgeons at our institution. The cohort size is relatively small, which prohibits rigorous statistical analysis for predictors of favorable outcome and complications. Without an equivalent cohort of non-embolized AVMs or nidi embolized with other agents, we are unable to assess the comparative effectiveness of SPE. Additionally, we are unable to determine if specific angioarchitectural patterns or nidus morphologies are more suited for devascularization with SPE. Larger cohorts of preoperative SPE of AVMs with longer follow-up durations are needed to fully characterize the role of this approach in the modern management of AVM patients.
CONCLUSION
In our experience, preoperative AVM embolization with silk suture and PVA particles affords a reasonable risk to benefit profile. Although larger studies are necessary to define the role of these embolic agents in the overall management of AVMs, we believe they can be employed with relative technical ease and favorable clinical safety prior to surgical extirpation of nidi in appropriately selected patients.
 XML Download
XML Download