

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primitive basilar carotid anastomoses form early during fetal embryogenesis. In the 4-mm human embryo, the internal carotid arteries extend from the paired dorsal aortic arches and anastomose at 3 major sites with the paired longitudinal neural arteries that constitute the primitive vertebro-basilar system in the hindbrain.6) From cephalic to caudal, these anastomoses affect the trigeminal, otic, and hypoglossal arteries, named according to adjacent structures.10) Ordinarily, these arteries regress and disappear by the fourth week of embryogenesis, beginning with the otic artery, followed by the hypoglossal, and finally, trigeminal arteries. Failure of these vessels to regress during embryonic development results in various persistent carotid-basilar anastomoses. Persistent primitive trigeminal artery (PPTA) is the most common carotid-basilar anastomosis, with an incidence between 0.1% and 0.6%.14) The least common anastomotic connection is persistent primitive otic artery (PPOA), which occurs in roughly 0.001% of the population.10)16)
We reported a case of PPTA that appeared similar to PPOA on cerebral angiography.
CASE REPORT
A 52-year-old woman was hospitalized with sudden-onset mental deterioration. An initial computed tomography scan showed an acute subarachnoid hemorrhage. Emergent cerebral angiography was performed, which led to a diagnosis of a ruptured aneurysm in the right middle cerebral artery bifurcation and 2 other unruptured aneurysms in the left middle cerebral artery bifurcation and left distal anterior cerebral artery bifurcation (A2-3). The patient immediately underwent surgical clipping. One month later, she was in full recovery. Later, surgical clipping and coil embolization were performed for the unruptured cerebral aneurysms.
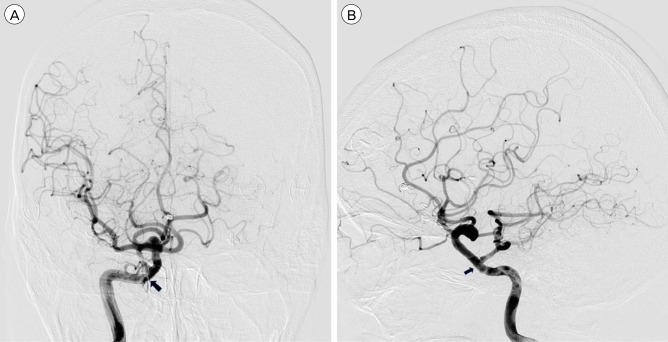
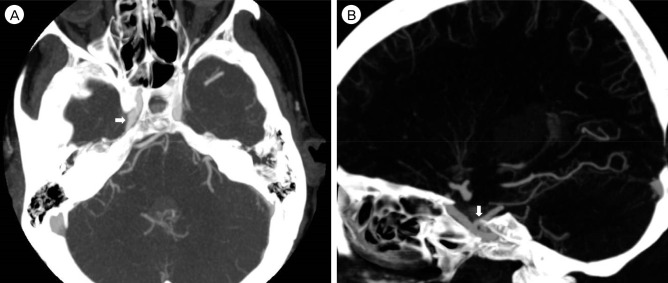
On cerebral angiography, we found a carotid basilar anastomosis that seemed to arise from the petrous segment and join with the middle basilar trunk (Fig. 1A, B). This vessel supplied blood to the regions of the distal basilar artery, contralateral posterior cerebral artery, and both superior cerebellar arteries. The ipsilateral posterior cerebral artery was supplied by a fetal type of posterior communicating artery. We first diagnosed this condition as persistent primitive otic artery because of its appearance on cerebral angiography. However, on brain computed tomography angiography (CTA) performed to identify the origin and course of the abnormal artery (Fig. 2A, B), we identified the origin of the abnormal artery as the petrocavernous junction. On CTA, this vessel was seen to originate from the lateral wall of the carotid artery, course posterolaterally with the trigeminal nerve through Meckel's cave, and insert into the basilar artery in parallel with the internal acoustic meatus. Based on the brain CTA images, we made a diagnosis of lower-lying PPTA.
DISCUSSION
PPTA was initially described by Quain.13) The trigeminal artery is most commonly associated with carotid basilar anastomoses. Their incidence is between 0.1% and 0.6%.14) The most common site of origin of PPTA is the posterior bend or lateral wall of the intracaverous carotid artery. A PPTA runs along the trigeminal nerve, enters the posterior fossa through Meckel's cave or the isolated dural foramen, and directly supplies blood to the cerebellum. The proximal basilar artery (BA) often shows some degree of hypoplasia with or without hypoplasia of the vertebral artery.2) Proximal hypoplastic BA below the point of abnormal communication and enlargement above is caused by hemodynamic changes in the posterior circulation distal to the connection point between the PPTA and the BA. Our case resembled that description. Understanding the presence and course of PPTA is clinically important. PPTA may be associated with intracranial aneurysms in 14-32% of cases.1)5) The reason for the frequent coexistence of intracranial aneurysms with PTA has been explained by the presence of structural defects in the walls of the cerebral arteries. Also, other associated vascular anomalies, such as VB insufficiency, arteriovenous anomalies, arteriovenous fistulas, and Moyamoya disease have been reported.3)7)8)11) Our case of SAH due to a ruptured aneurysm associated with a lower-lying PPTA and concomitant multiple aneurysms is rare.
The existence of PPOA is still controversial, because PPOA has never been identified in lower organisms.9) Nevertheless, there have been a few reports of PPOA. PPOA, if it exists, is thought to arise from the petrous internal carotid artery within the carotid canal, course laterally through the internal auditory canal, and anastomose with the proximal basilar artery.10) It is unclear whether previously reported cases of PPOA are true PPOA or, instead, lower-lying PPTA or stapedial artery remnants because the poor quality of images and the presence of a single angiographic picture in the published reports makes it difficult to be sure of the origin, course, and junction site of the vessels. Croft suggested that a true otic artery has not yet been reported.4)
In our case, a carotid basilar anastomosis with coexisting multiple aneurysms was identified on cerebral angiography. At first, this vessel appeared to arise from the lateral petrous internal carotid artery and course parallel to the internal auditory canal. However, using brain CTA, we concluded that this vessel originated from the internal carotid artery at the outlet of the carotid canal. Thus, brain CTA is useful in evaluating the relationship between the vascular anatomy and surrounding bony structures. Finally, we were able to diagnose the abnormal artery as a lower-lying PPTA and not PPOA. Several previous case reports on PPOA did not clearly demonstrate the origin, course and termination of anastomoses.4)12)15) Therefore, based on our experience, it seems that brain CTA is needed to definitively diagnose the type of carotid-basilar anastomoses.
 XML Download
XML Download