

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Endovascular treatment for large and giant cerebral aneurysms, which generally have wide necks, is often performed using a stent to preserve the parent vessel.1)2)3)4)6) Microcatheter navigation into a distal vessel across the aneurysm neck enables stent deployment and various microcatheter navigation techniques are available to accomplish this.1)2)3)4)6) However, the microcatheter may again protrude the aneurysm during the stent navigation process after microcatheter advancement into the distal vessel across the aneurysm neck. Here, we report a case of successful open-cell stent deployment across the wide neck of a large middle cerebral artery (MCA) aneurysm using the stent anchor technique.
CASE REPORT
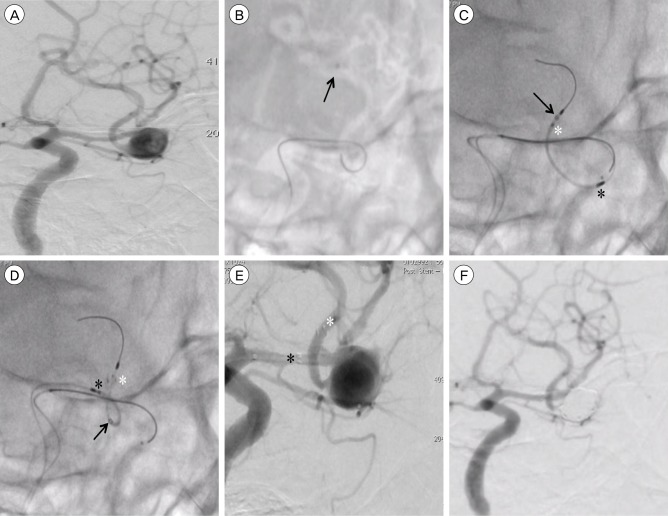
A 56-year-old man consulted outpatient department on foot 7 days after the sudden onset of headache. Magnetic resonance imaging showed a subarachnoid hemorrhage (SAH) and an MCA aneurysm. A three-dimensional rotational digital subtraction angiogram (DSA) of the left internal carotid artery (ICA) showed a large (8.0 × 13.0 × 11.5 mm) MCA aneurysm with an 8.0 mm-wide neck in the MCA bifurcation with a 2.7 mm inferior M2 branch arising from the aneurysm body (Fig. 1A). The patient and his relatives preferred endovascular treatment over surgical clipping; therefore, we performed the former.
Antiplatelet drugs including clopidogrel 300 mg and aspirin 200 mg were given for the stent-assisted coil embolization. The procedure was performed under general anesthesia. A 6-Fr 90 cm guiding sheath (ASAHI FUBUKI Dilator; Asahi Intecc, Aichi, Japan) was placed into the left ICA via the femoral artery. The activated clotting time was maintained at ≥ 250 s by the intravenous administration of heparin during the procedure.
An Excelsior XT-27 Flex microcatheter (Stryker Neurovascular, Fremont, CA, USA) over a CHIKAI black microwire (Asahi Intecc) was looped in the aneurysm and navigated into the left inferior MCA branch. The loop of the microcatheter in the aneurysm was then straightened using gentle traction on both the microcatheter and the microwire (Fig. 1B). An Excelsior SL-10 microcatheter (Stryker Neurovascular) was placed within the aneurysm using a jailing technique.
When a NeuroformEZ3 Stent System (4.0 × 20 mm; Stryker Neurovascular) was advanced across the aneurysm neck through the microcatheter, the microcatheter again protruded into the aneurysm due to the sharp bend of the microcatheter and the stiffness of the stent (Fig. 1C). Our attempt to reduce and straighten the loop by gently withdrawing the microcatheter failed.
Therefore, the stent was partially deployed distal to the aneurysm neck with the stent obtaining purchase within the distal vessel lumen. Next, the loop of the microcatheter in the aneurysm was withdrawn slowly by anchoring of the partially deployed stent (Fig. 1D). The stent was then completely deployed across the aneurysm neck (Fig. 1E). After successful stent deployment, coil embolization was performed using the jailed microcatheter. The DSA performed at the conclusion of the procedure revealed complete aneurysm obliteration (Raymond scale 1) with patency of the inferior M2 branch (Fig. 1F). The patient had no new neurological deficits. One month after the onset of the SAH, the patient was discharged with a modified Rankin Scale score of 1.
DISCUSSION
In distal artery navigation of a microcatheter for stent deployment, the microcatheter was often navigated into the distal vessel by looping within the aneurysm. On the other hand, in a giant aneurysm, the microcatheter was navigated into the distal vessel without a looping in the aneurysm after the balloon is inflated inside the aneurysm and made to seal the neck orifice of the aneurysm.4)
Then, the loop of the microcatheter in the aneurysm have been straightened by several techniques.1)2)3)4)6) In the balloon and coil anchor technique, the loop of the microcatheter in the aneurysm is straightened by the anchoring of a balloon and a coil in the distal vessel across the aneurysm neck.1)6) Without a balloon or coil, the loop of the microcatheter in the aneurysm is straightened by traction applied to both the microcatheter and the microwire.2) Furthermore, in the previously reported stent anchor technique, the loop of the microcatheter in the aneurysm is straightened by the anchoring of a partially deployed closed-cell stent (Enterprise stent: Codman Neurovascular, Johnson & Johnson, Miami, FL, USA) distal to the aneurysm neck to enable direct stent deployment.3)
Self-expanding intracranial stents are open- or closed-cell by design.5) Open-cell stents such as the Neuroform provide good apposition to the curvature of the vessel wall, but they are non-re-sheathable.5) Closed-cell stents such as the Enterprise are re-sheathable but feature poor apposition to the vessel wall. An in vitro examination revealed that the Neuroform stent had a higher outward radial force and better wall apposition than the Enterprise stent.5) Therefore, the fixation to the distal vessel and apposition to the sharp bend of the branching artery arising from the aneurysm body may be better suited to treatment using the Neuroform stent than the Enterprise stent.
In the present case, stent deployment across the aneurysm neck was performed using the stent anchor technique because the microcatheter again protruded into the aneurysm during the stent navigation. An open-cell stent was used as the anchor due to the sharp bend of the M2 branch arising from the aneurysm body and was very carefully deployed despite its risks of intra-aneurysmal stent migration and difficulty in recovery from stent malposition due to non-re-sheathable nature. But, that technique could be bring about such dangerous or unwanted events as intrasaccular microcatheter and stent herniation with/without the aneurysmal perforation when crossing the aneurysm neck. Therefore, intrasaccular coil embolization before deploying a stent across the aneurysm neck would be necessary. And also, open-cell stents in the stent anchor technique could induce vessel wall damage, compared with closed cell stents. Even if the microcatheter was navigated into the distal vessel across aneurysm neck, it might protrude into the aneurysm during the stent navigation process due to the sharp bend of the microcatheter as in this case. Therefore, the stent anchor technique may be useful for stent deployment in cases of microcatheter protrusion into the aneurysm during the stent navigation.
 XML Download
XML Download