

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Age is an important risk factor for stroke occurrence.
Approximately 30% of acute strokes occur in those
older than 80 years of age.6)9)24) However, elderly patients
tend to have high rates of poor outcomes and
in-hospital mortality.1)4)8)13)14)16)17)23)25)26)30) Furthermore, family members of elderly patients are often reluctant to accept aggressive treatment. Recently, prospective trials have shown the benefit of endovascular treatment (EVT) for acute ischemic stroke.5)12)20)22)32) However, some trials included only patients aged 80 or less,20)32) and although trial inclusion criteria had no age limitation, a small proportion of elderly patients over 80 years were included.5)12)22) Therefore, the evidence supporting that endovascular treatment can be actively recommended for elderly patients as for younger patients is not sufficient.
To determine whether EVT for acute ischemic stroke is also beneficial in acute ischemic stroke patients over 80 years of age who are candidates for EVT, outcomes were compared between patients who underwent EVT and those who did not, in terms of functional outcomes and rates of symptomatic hemorrhage, in-hospital morbidities, and mortality.
MATERIALS AND METHODS
Patient Selection
This retrospective study was approved by our Institutional Review Board. From a stroke registry (January 2009-March 2014) at our institution, data was collected on patients matching the EVT criteria for acute ischemic stroke of our institution: (1) time from onset < 8 hours, (2) major artery occlusion (internal carotid artery, middle cerebral artery [M1 and M2], basilar artery, or vertebral artery), (3) diffusion-perfusion mismatch on MRI (> 120% difference between diffusion weighted imaging and time to peak map), (4) an initial National Institute of Health Stroke Scale [NIHSS] score of ≥ 5, and (5) within time from onset of 4.5 hours, no clinical response to intravenous tPA, as described in previous studies.21)28) Patients who had intracranial hemorrhage, large infarctions (infarction size on diffusion MRI ≥ 1/3 on middle cerebral artery territory), bleeding diathesis, or serious illnesses affecting life expectancy including malignancy were excluded.
For 478 patients matching the EVT criteria retrieved from the registry, additional criteria were applied: age > 80 years and a prestroke modified Rankin Scale (mRS) score of ≤ 2. A total of 156 patients were selected as study subjects. To ensure agreement with the above mentioned criteria, the clinical and radiologic data of the patients were re-reviewed by two investigators (K.H. and C.H.K.). The stroke MRI protocol and the method of measuring diffusion-perfusion mismatch used have been previously described.18)
Patient management
At our institution, intravenous (IV) administration of tissue plasminogen activator (tPA) is considered, regardless of patient age, when indicated. Accordingly, of the 156 study subjects, tPA was administered in 95 patients matching IV tPA indication, but none of them showed a clinical response. In the remaining 61 patients, IV tPA was not used, from passing its time window in 58 patients or from a previous history of intracranial hemorrhage in 3 patients.
Unlike IV tPA administration, EVT for patients over 80 years of age was not actively recommended during the study period. Information on risks and benefits of EVT was provided to first-degree family members (spouse, sons, and daughters) and EVT was performed when they agreed. Because none of the patients were clearly conscious, they were unable to participate in this decision. Of the 156 study subjects, family members of 100 (64.1%, non-EVT group) patients refused EVT, thus they received standard medical treatment in the stroke unit in accordance with stroke guidelines.19) The remaining 56 (35.9%, EVT group) patients underwent EVT according to agreement of family members. In line with our EVT protocol, we primarily used clot retrieval using a Penumbra reperfusion catheter (Penumbra, Alameda, California) or a Solitaire FR stent (ev3, Plymouth, Minnesota). Intra-arterial infusion of fibrinolytics was reserved for cases with a remaining small amount of thrombi or distal migrating emboli. Technical details have been previously described.3)21)28) After EVT, they were also managed according to the standard treatment guidelines in the stroke unit.
Data collection
Basic demographic and clinical data (past history, occlusion site, Trial of Org 10172 Acute Stroke Treatment [TOAST] classification, time from onset, initial NIHSS score, IV tPA use, hemorrhage, in-hospital mortality, and mRS score [prestroke, and at 3 and 12 months after stroke]) were retrieved from the stroke registry. According to the criteria proposed by the European Cooperative Acute Stroke Study (ECASS) group,15) hemorrhage was classified as: hemorrhagic infarction type 1 (HI-1), hemorrhagic infarction type 2 (HI-2), parenchymal hematoma type 1 (PH-1), or parenchymal hematoma type 2 (PH-2). Symptomatic hemorrhage was defined as one associated with a ≥ 4-point increase in NIHSS score or a 1-point deterioration in level of consciousness.11) The stroke registry was controlled by two stroke neurologists (H.J.B. and M.K.H.). Discrepancies were resolved by consensus during weekly registry meetings.
In-hospital morbidities, including the need for endotracheal intubation, gastrointestinal bleeding, pneumonia, and urinary tract infection (UTI), were obtained by review of medical records (S.P.B. and B.L.). Gastrointestinal bleeding included hematemesis and melena. Patients were considered to have a hospital-acquired infection, when they had clinical, radiological, and laboratory findings compatible with infection and the organism was confirmed by culture.
The angiographic outcomes of patients who underwent EVT were reviewed and graded by two neurointerventionists (G.H. and O.K.K) using Thrombolysis in Cerebral Ischemia (TICI) grades. Successful recanalization was defined as a TICI grade of ≥ 2b. All complications that occurred during EVT were documented.
Measurement of the Effects of EVT
The effects of EVT were determined using: (1) good functional outcome (defined as a mRS score of 0-2) rates at 3 and 12 months after stroke, (2) symptomatic hemorrhage rates, (3) in-hospital morbidity rates (endotracheal intubation, gastrointestinal bleeding, pneumonia, and UTI), and (4) in-hospital mortality rates.
Statistical analyses
Statistical analysis was performed using STATA (version 13, STATA Corp LP, College Station, TX). The Mann-Whitney U test was used for bivariate analysis of continuous variables and the χ2 or Fisher's exact test for bivariate analysis of nominal factors. The effects of EVT were compared using binary logistic regression analysis, adjusted for confounders significantly associated with outcome after ischemic stroke: age (< 85 or ≥ 85 years), time from onset (< 4.5 or 4.5-8 hours), initial NIHSS score (moderate, 5-14 or severe, ≥ 15), and prestroke mRS score (0 or 1-2). "tPA use" was excluded from the logistic regression models, because of a lack of clinical response after tPA use in all cases and correlation with time from onset causing a multicollinearity problem. Two-sided probability values of < 0.05 were considered to indicate statistical significance.
RESULTS
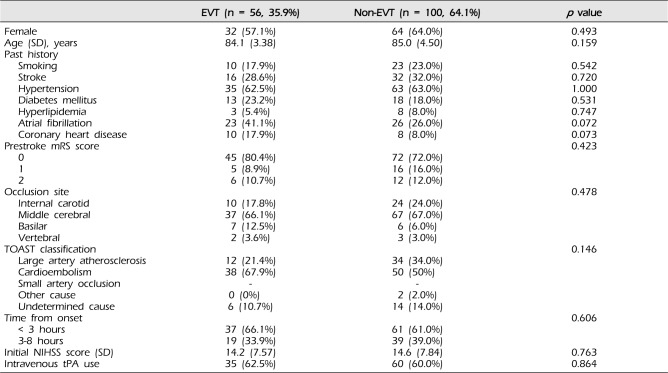
Basic demographic and clinical data were not significantly different in the EVT and non-EVT groups (Table 1). In the EVT group, successful recanalization (TICI grade ≥ 2b) was achieved in 46 patients (82.1%). Of these, 25 patients did not achieve good outcomes and thus, futile recanalization, defined as mRS ≥ 3 despite successful recanalization, was 54.3%. Complications occurred in 3 (5.4%) patients during EVT: vessel rupture in 2 patients and intracranial artery dissection in 1 patient. Of these, good outcomes were achieved in 2 patients at 3 and 12 months after stroke. Recanalization failed in 1 patient with vessel rupture, whose outcome was poor (mRS 5 at 3 and 12 months), although bleeding was stopped by temporary balloon occlusion.
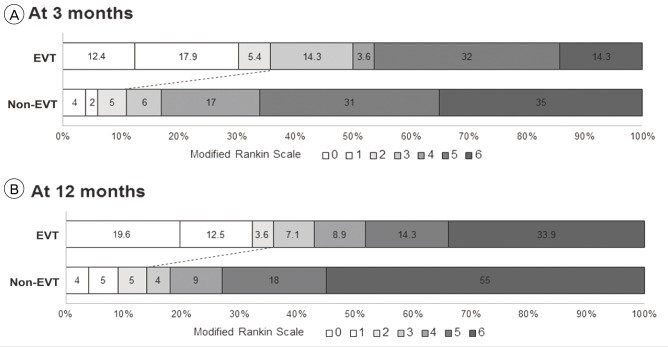
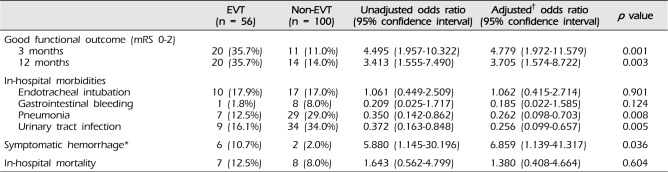
At 3 months after stroke, good functional outcomes were achieved in a greater portion of patients in the EVT group than in the non-EVT group (20 [35.7%] vs. 11 [11.0%], adjusted odds ratio [OR] 4.779, 95% confidence interval [CI] 1.972-11.579, p = 0.001; Table 2 and Fig. 1A). At 12 months follow-up, this trend continued and the good functional outcome rate was significantly higher in the EVT group than in the non-EVT groups (20 [35.7%] versus 14 [14.0%], adjusted OR 3.705, 95% CI 1.574-8.722, p = 0.003; Fig. 1B). In the non-EVT group, proportions of patients who were severely disabled or dead (mRS score of 4-6) were over 80% and significantly higher than in the EVT group at 3 months (83 [83.0%] vs. 28 [50.0%], adjusted OR 6.950, 95% CI 2.844-16.985, p < 0.001) and 12 months (82 [82%] vs. 32 [57.1%], adjusted OR 4.180, 95% CI 1.837-9.510, p = 0.001) after stroke (Fig. 1A, B).
Of in-hospital morbidities, pneumonia (7 [12.5%] versus 29 [29.0%], adjusted OR 0.262, 95% CI 0.098-0.703, p = 0.008) and UTI (9 [16.1%] versus 34 [34.0%], adjusted OR 0.256, 95% CI 0.099-0.657, p = 0.005) were significantly less frequent in the EVT group during admission (Table 2).
Hemorrhage occurred in 40 (25.6%) patients, including 8 (5.1%) with symptomatic hemorrhage during admission. Although hemorrhage types (HI, 6 [10.7%] vs. 11 [11.0%]; PH, 9 [16.1%] vs. 14 [14.0%], p = 0.941) were similar in the two groups, symptomatic hemorrhage rates were significantly higher in the EVT group (6 [10.7%] vs. 2 [2.0%], adjusted OR 6.859, 95% CI 1.139-41.317, p = 0.036).
In-hospital mortality rate did not differ significantly between the EVT and non-EVT groups (7 [12.5%] vs. 8 [8.0%], adjusted OR 1.380, 95% CI 0.408-4.664, p = 0.604).
DISCUSSION
The present study shows that EVT for acute ischemic stroke was associated with good functional outcomes at 3 and 12 months after stroke in patients over 80 years of age who were candidates for EVT. It also reduced rates of in-hospital morbidities, such as hospital-acquired infections. Although symptomatic hemorrhage occurred more frequently after EVT, overall functional outcome of elderly patients treated by EVT was still better and in-hospital mortality rate was not higher than that of patients not treated with EVT.
Our results indicate that the benefit of EVT for acute ischemic stroke is maintained even in patients over 80 years of age. Therefore, elderly patients should not be simply excluded from EVT candidates because of their age. This is consistent with subgroup analysis of recent prospective trials reporting that no significant interaction was detected between the benefit of EVT and age.5)12)
In addition to functional outcomes, in-hospital morbidities were also evaluated as a primary outcome of EVT, because these often lead to unfavorable or fatal outcome in elderly patients.8)13) We found that pneumonia and UTI developed more frequently in the non-EVT group. Poor clinical condition in patients with acute ischemic stroke is associated with these in-hospital morbidities and, in turn, their developments are predictors for unfavorable outcome and mortality.2)7)10)27)29)31)33)34)35)36) Therefore, these findings suggest that a better clinical condition achieved by EVT would reduce in-hospital morbidities, contributing to a more favorable outcome in EVT groups.
Symptomatic hemorrhage is an important complication associated with thrombolysis for acute ischemic stroke. Especially in elderly patients with acute ischemic stroke, symptomatic hemorrhage is frequent and associated with high rates of in-hospital mortality and poor outcome.1)4)8)13)14)16)17)23)25)26)30) In the current study, however, in-hospital mortality rates were not different between the two study groups. In addition, more than 80% of patients not treated by EVT were severely disabled or dead (mRS score of 4-6) due to acute stroke or its sequelae at 3 and 12 months after stroke, thus this proportion was found to be much higher than that of the EVT group. Therefore, these results indicate that the benefit of EVT overweighs the risk of symptomatic hemorrhage after EVT.
In practice, we frequently encounter elderly patients with acute ischemic stroke, but no consensus has been reached on this issue. Although our results do not provide definite evidence obtained from a well-designed randomized study, we believe that they could provide some useful information for physicians and patients, until sufficient data become available.
Several limitations of the current study should be addressed. These include its retrospective nature, single center experience, and its relatively small cohort. In addition, selection bias is likely to have been introduced by involving family members in the treatment decision-making process, and the general management afforded to both EVT and non-EVT groups may have been less than aggressive due to considerations of patient age. Nevertheless, the general management guidelines followed were identical for the EVT and non-EVT groups and all patients were managed without abandoning treatment, because only patients whose family-members agree on treatment for stroke are permitted to be referred to our tertiary referral hospital.
CONCLUSION
The present study demonstrated that EVT improved functional outcomes at 3 and 12 months after stroke in patients over 80 years of age with acute ischemic stroke who were candidates for EVT. It also reduced rates of hospital-acquired infections. These results indicate that the benefit of EVT for acute ischemic stroke is maintained in elderly patients. In these patients, symptomatic hemorrhage occurred more frequently after EVT, but the benefit of EVT overweighs the risk of symptomatic hemorrhage, considering the high rate of poor outcomes in patients who did not undergo EVT. Accordingly, our findings suggest that EVT can be considered in elderly patients, if indicated.
 XML Download
XML Download