

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Due to improvements in non-invasive imaging, detection of a number of incidental aneurysms is increasing, and management of unruptured intracranial aneurysms has changed significantly in recent years and continues to evolve. In particular, the establishment of endovascular therapy as an attractive alternative to surgery has prompted significant changes in neurosurgical practice.
Management of middle cerebral artery aneurysms (MCAA) is a challenge for neurosurgeons. Although endovascular treatments may be effective for some MCAA,1) most neurosurgeons have favored microsurgical clipping.9) Most surgeons utilize the conventional pterional approach for MCAA surgery. However, contrary to ruptured aneurysm, surgery of incidental MCAA is possible by opening of the distal sylvian cistern without opening of the carotid cistern and proximal sylvian cistern because the MCAA is located near the brain cortex. The authors performed clipping of incidental MCAA through a small temporal craniotomy and linear scalp incision instead of the standard pterional approach. We introduced this new approach and reported the results.
MATERIALS AND METHODS
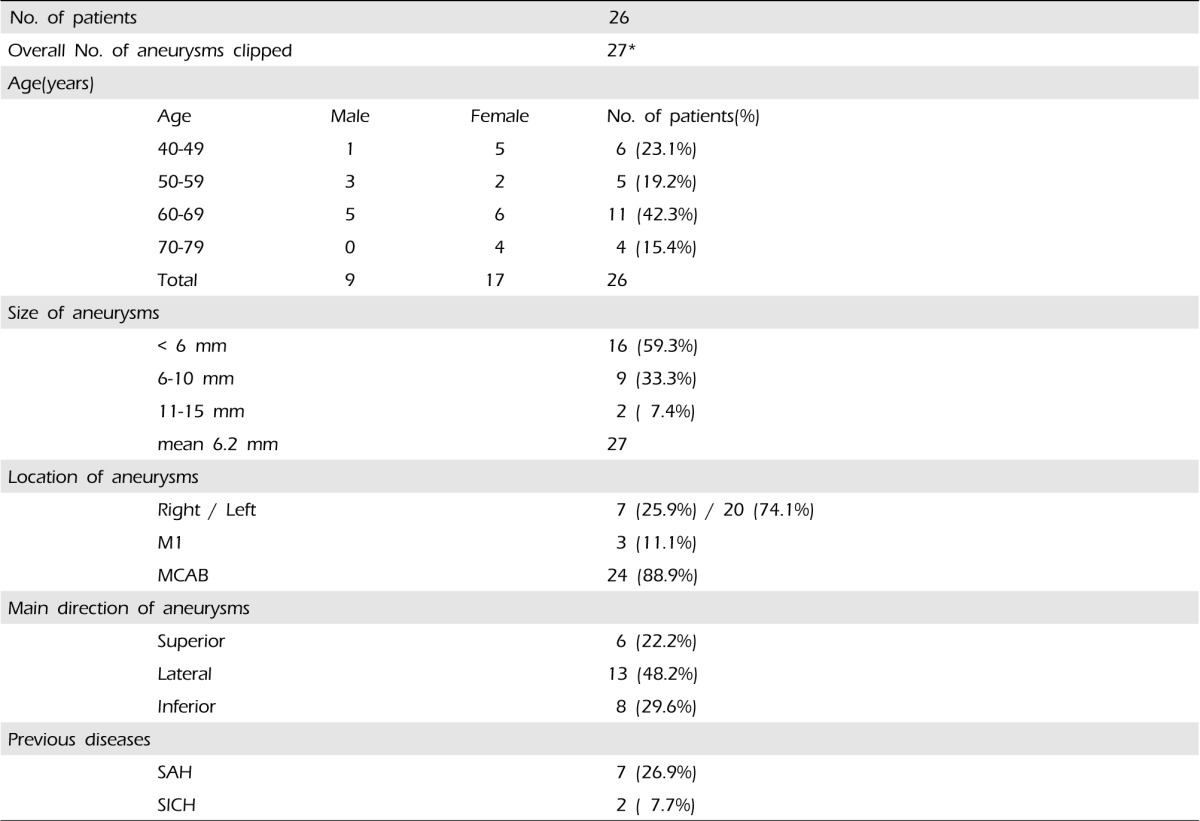
We retrospectively reviewed 26 patients with unruptured MCAA treated by clipping through a small temporal craniotomy and a linear scalp incision from January 2010 to December 2012. A list of patient demographic data and characteristics of the aneurysm is shown in Table 1. Size and main directions, locations of aneurysms were checked by conventional computed tomography (CT) angiography. One of 26 patients had multiple aneurysms: MCA bifurcation aneurysm and M1 segment aneurysm. Seven patients had a previous history of surgery for other aneurysms: anterior communicating artery (Acom) and contralateral MCA in two cases, Acom and contralateral MCA, superior cerebellar artery (SCA) in one case, and contralateral MCA aneurysm in four cases. Two patients had a history of treatment for spontaneous intracerebral hemorrhage (SICH).
SURGICAL TECHNIQUE
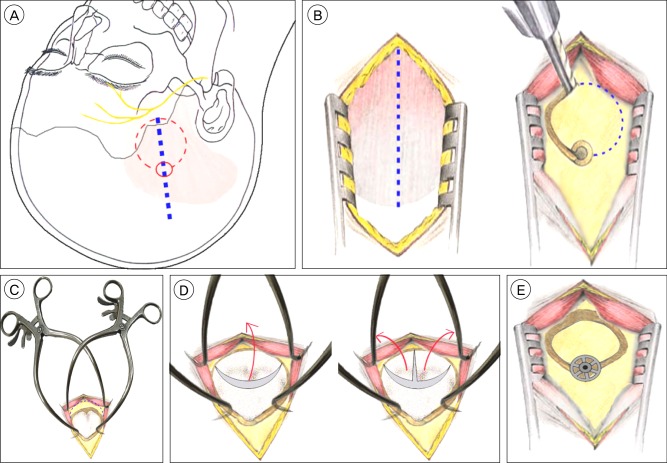
Patients were placed in the supine position with head rotation to the opposite site 60 degrees. Saving of scalp hair and use of skull cramps were not necessary. To prevent injury to the frontal branch of the facial nerve, skin incision began from 1 cm below the anterior temporal hair line and extended upward to the parietal eminence (Fig. 1A).
The temporalis muscle was cut with a knife along the incision line and stripped from its bony insertion and was retracted bilaterally. Using a high-speed drill, a single temporal burr hole was drilled and a "O" shaped line was cut from the burr hole using a high-speed craniotome, creating a bone flap with a width of 4×4 cm (Fig. 1B). After removal of the bone flap, the sphenoid ridge was flattened using a high-speed drill. For maximal resection of the sphenoid ridge, we utilized two Gelpi retractors. One side of the Gelpi retractors was located to the bony margin of craniotomy and the other side to the temporalis muscle (Fig. 1C).
The dura mater was opened in a curved or "inverted T" shaped fashion with its base toward the remnant sphenoid ridge. The free dural flap was fixed downward with sutures (Fig. 1D) and the posterior part of the inferior frontal gyrus and superior temporal gyrus, distal sylvian fissure were exposed.
Under microscopy, the first step was the sufficient evacuation of cerebrospinal fluid (CSF) at the distal sylvian fissure. Once the distal sylvian fissure was opened, the MCAA usually came into view. However, in cases of M1 segment aneurysm and short segment of MI, wider dissection of the sylvian fissure was inevitable. Without exposure of the feeding artery to the aneurysm, the aneurysm was freed from adjacent tissue directly and aneurysmal clipping was performed.
The bone flap was fixed with a titanium Craniofix miniplate. The burr hole was closed with the plate (Fig. 1E). The temporalis muscle and superficial temporalis fascia were reattached directly. Use of a suction drain was not necessary.
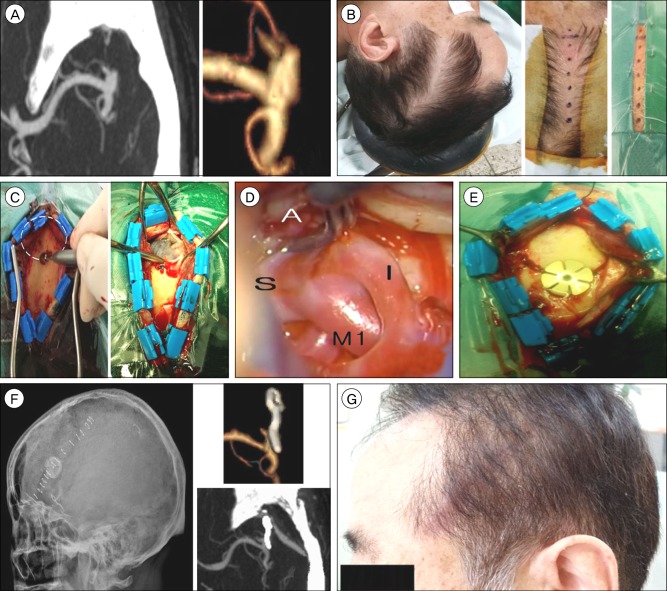
CASE REPORT
A 60-year-old male patient presented with headache. CT angiography showed a left MCA bifurcation aneurysm; an unruptured saccular type aneurysm measuring 6×4 mm in size. The patient was treated by clipping via a small temporal craniotomy and linear scalp incision and recovered well without any complications (Fig. 2A-G).
RESULTS
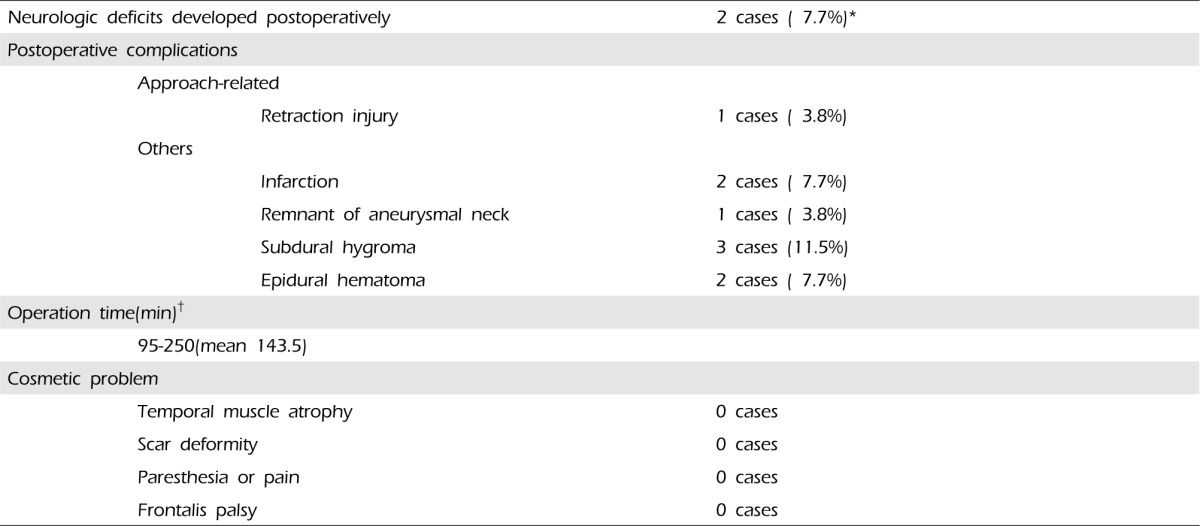
Complications were classified according to two categories: approach-related and others (Table 2). Approach-related complication was retraction injury in one of 26 cases (3.8%). Postoperative follow up CT showed focal low density on the temporal cortex, which was assumed to be a retraction injury and neurologic deficits not developed as a result of the retraction injury.
Two patients developed postoperative infarction: on the left MCA territories and left cerebellum. Infarction of left MCA territories was due to vasospasm of the MCA and infarction of the left cerebellum unrelated to this approach. Two patients with infarction were discharged with some remnant neurologic deficit.
Follow-up images showed complete occlusion of 26 aneurysms (96.3%), residual neck in one (3.7%). Residual neck of the aneurysm had not grown on serial follow up.
There were minor complications, including a small amount of epidural hematoma in two cases and subdural hygromas in three cases on postoperative brain CT, which did not require evacuation. Operation time was checked by taking the time from scalp incision to close time, 95 min-250 min (mean 143 min).
The cosmetic results of this approach were excellent. There were no temporal muscle atrophy, scar deformity, paresthesia or pain around the scalp incision, frontalis palsy.
DISCUSSION
The modern conventional pterional craniotomy was first introduced by Yasargil and Fox in 1975.13) Since then, various modified approaches have been introduced. Even with the advent of new approaches,3)4)5)12) the pterional craniotomy is most commonly used because it offers a broader base of surgical field, and can be performed with minimal surgical morbidity and mortality.
However, the pterional approach could increase both operation time and surgical morbidity because of wide exposure with a long skin incision, splitting of the temporalis muscle, large craniotomy, and drilling of the sphenoid ridge.5)7) Risks of facial nerve damage, temporal muscle atrophy, paresthesia and pain along the incision scar and cosmetic bony defect can also increase.2)11)14) The authors devised a new approach for incidental MCAA surgery without the long incision and large craniotomy of the pterional approach. Contrary to ruptured aneurysms, clipping of incidental MCAA is possible by opening of the distal sylvian cistern without dissection of the carotid cistern and proximal sylvian cistern. The reasons are as follows: 1) unnecessary removal of subarachnoid hemorrhage (SAH), 2) absence of brain swelling, 3) easy evacuation of CSF for brain slackening, 4) location closer to the brain cortex than other aneurysms within the intracranial circulation, 5) unnecessary exposure of proximal MCA for temporary clip occlusion.
Compared to the pterional approach, this approach certainly offers several advantages due to much smaller craniotomy and shorter skin incision. Therefore, use of this approach can achieve short surgery time, minimal injury of temporalis muscle, decrease in blood loss, good cosmetic result, and no injury to the frontal branch of the facial nerve.
However, a major drawback of this approach is the problems that can occur because of the narrow operative window, which is a non-issue in surgery of a typical MCAB aneurysm. Yet cases of M1 aneurysm and/or short M1, buried aneurysm to the temporal lobe or frontal lobe, complex aneurysm with a large size, and severe atherosclerosis require more retraction of the frontotemporal lobe and wide dissection of the sylvian cistern, and retraction injury of the frontotemporal lobe and sacrifice of the main sylvian vein can occur. Therefore, this approach is a contraindication in cases mentioned above.
The most important principle in an aneurysm surgery is to secure the afferent artery prior to the aneurysm exposure. However, it is not absolutely indispensable to an unruptured aneurysm. In this approach, first, the top of the aneurysm is exposed and it will be difficult to secure the artery feeding the aneurysm, namely the M1 portion. Hemorrhage due to aneurysm rupture is difficult to control under such circumstance. Fortunately, such complications did not occur in this study. Other noteworthy points of this approach are inadequate placement of the craniotomy and injury of the frontalis branch of the facial nerve. The optimal placement of craniotomy can be effectively controlled with the use of modern navigation tools. The latter can prevent damage of the frontalis branch by avoiding skin incision beyond the lower part of the anterior temporal hair line.6)13)
In two patients who developed postoperative infarctions, neurologic deficits exist. In one of the two patients who underwent surgery for contralateral MCA aneurysmal rupture 40 days ago, postoperative infarction on MCA territory occurred because of vasospasm. We should take a more delayed approach to surgery. In another case, postoperative infarction of the left cerebellum occurred independently of this approach. Strictly speaking, they were not approach-related complications.
Safety and long term efficacy are the goals of treatment of unruptured aneurysms.8) The authors obtained excellent results using this approach. However, we object to use of this small and restricted craniotomy to address most unruptured MCA aneurysms, particularly if they are large and/or complex and deep-seated. Working through a small craniotomy such as this approach, the surgeon is confined to a narrow angle of vision, and the ability to address complex situations is more limited than with the broader base afforded by a standard pterional craniotomy.10) First, the majority of neurosurgeons should consider safety and good results rather than the size of the incision or the bone flap. Experienced operators can use this approach safely and will obtain excellent results by selection of an adequate indication to this approach.
 XML Download
XML Download