

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Menopause is the time of a woman's life when her periods permanently stop. It ovary stops to produce estrogen and progesterone hormones and cancels the women's power of reproducing. The age range of 45 to 55 years is known as natural menopausal time of worldwide women.1 But in Bangladesh the maximum range is up to 55 years.2 If any woman's period stops before 45 years old is called early menopause3 and if after 50 years old is called as late menopause in this research. After the change of period the women face many physical problems as well as psychosocial problem.45 Important impacts in the daily, social and sexual life of postmenopausal women have to faces for menopause.678 The number of health criteria changed rapidly in her body like tiredness, sleeping problem, hot flashes, hair loss, sweats etc.
The average life range of women in Bangladesh is 60 to 65 years. Many women are likely to live for more than 15 to 20 (One third of life) years after menopause. For decreasing energy and increasing physical as well as mental problems those women are considered as risk population.9 So 35 to 45 years old women's health issue is the most public health concerning topic around the world. World Health Organization defines quality of life (QOL) whose essential component in clinical practices is to study about early menopausal women. QOL conducted with early menopausal women of developed countries by different sociocultural realities. But QOL holds very little information about early menopausal women of developing countries.10
It is well documented that every menopausal symptoms have effect on QOL of menopausal women.11 Every menopausal symptoms impact on lifestyle is not same. It varies from one region to another as well as one country to another according to their culture. It is observed that a significant variation is present among western menopausal women, North American menopausal women, European menopausal women and Asian menopausal women. Bangladesh is a developing country in South East Asia. Most of the women are uneducated and have no consciousness about menopausal symptoms effect on quality of life. Some women's menopause stops early before 45 years and some late after 51 years. Both cases women have to face menopausal symptoms impact on life. But there is no documentation about both early and late menopausal women of Bangladesh.
Like as western countries, menopausal symptoms have not been extensively studied in South East Asia12 including Bangladesh. So information is not available of developing countries in South East Asia like Bangladesh. This study aimed to document the menopausal related symptoms for both early and late menopausal women of Tangail region of Bangladesh. Another purpose of this study is to compare the QOL of both cases women.
Materials and Methods
1. Study population and data collection
This study is an ongoing multicenter population-based study to investigate the relationship among lifestyle factors of causing early and late menopause, type 2 diabetics and problem for abnormal menopausal time. Collected data consisted with 150 participants (all are women), enrolled into the recorded data between 2013 and 2014, in 3 study centers across 3 different palaces in Bangladesh (i.e. Santosh, Palpara, Goshpara in Tangail). In recorded data the majority participants were between 50 and 70 years old although recorded data hold 42 to 90 years old participants information. Pregnant, breast feeding, hormone therapy taken women, and women with uncontrolled medical conditions like type 2 diabetics, hypertension or coherent heart disease were participated in our cross-sectional study. Some participants gave written informed consent and others were in viva-voce, and the study was approved by the local committees at the participating centers and Department of Biotechnology and Genetic Engineering Research and Ethics Committee, Mawlana Bhashani Science and Technology University. With socio demographic information, menstruation status based data were reported according to the length of time since last menstrual period and the experience of symptoms on QOL.
At primary stage, questionnaires and computer-guided, face-to face interviews were used to record information about basic lifestyle, illness, problems for abnormal menopausal stage (early menopause or late menopause). Mainly literature review, exploratory research and qualitative piloting informed the development and refinement to structure a questionnaire in English. Questionnaire information on lifestyle covered lifetime history as well as current habits (at recruitment time) of physical activity without work, body mass index (BMI) in height (m) / weight (kg)2 where height and weight were measured by following standardized procedures. Although regular exercise is mentioned here as physical activity without work which makes man happy with good health and improves QOL. Besides, majority participants were not concerned about problems of BMI, only 15% were careful. The other information in questionnaire was close and open ended including series of questions whose are associated with abnormal menopausal factors such as age, blood pressure, hot flashes, osteoporosis, type 2 diabetics, coherent heart disease, heart beating, feeling tense or nervous, sleeping problem, excitable, concentrating problem, feeling tried or lacking in energy and dizzy, depression, physical problem (pain, backaches, bloating, sore breasts, headaches diarrhea, food cravings etc.) during menstruation, irritability, pressure or tightness in head or body, parts of body feel numb or tingling, headache, muscle and joint pain, loss of feeling in hands or feet, breathing problem, sweating at night etc. The answer of questions could be categorized as numeric number for age, height and weight factors, high or low for blood pressure factor, early or late for menopausal status factor and yes or no for rest of factors.
A total of 67% participants who had reported early menopausal status at the time of baseline recruitment and 33% participants were late menopausal status.
2. Data cleaning
As for collecting data from different places may carry duplicate and missing values which can help to provide wrong investigational result. So data cleaning (also known as data pre-processing) is a vital step not only for minimization of memory but also normalization of values what used to represent information in database. In this study duplicate values (1.33% in whole collection) were discarded and missing values (2% in whole collection) were provided according to other participants' information of those places. Finally 150 participants' data were enlisted for research study what was checked using Waikato Environment for Knowledge Analysis (WEKA) toolkit of 3.6.5 version.
3. Data mining and statistical analysis
The goals of research are to analyze early menopause and late menopause with association among factors (mentioned in questionnaire). With regard to menopausal status (goal) variables, study participants were categorized according to menopausal status at the time of recruitment (early, late). Subjects who reported early menopausal stage at baseline were further categorized by the lifestyle factors (dispersion, tiredness, sleeping problem etc.) and disease factors (hot flashes, osteoporosis, diabetics etc.) what happened for early menopause. Similar work was done for late menopause.
Participants were divided into quartile categories of BMI with gender (all are female) specific quartile cut points based on full collected data. The participants having BMI range (0-24, 25-28, 29+) categorized as (low, medium, high). The BMI range of category is selected through the diabetic's factors assessment for Bangladeshi population by Ahmed et al.13 The data were analyzed using MS Excel spread sheet 2010, WEKA of version 3.6.5. Using ranker algorithms the factors (both lifestyle and disease factors) were ranked for both menopausal status. Collected data were also analyzed using SPSS Version 20.0 software (SPSS, Inc., Chicago, IL, USA). Finally comparing WEKA and SPSS result enlisted the most significant lifestyle and disease factors.
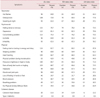
In statistical analysis, to evaluate the quality of life of women with menopausal symptoms, different techniques were used in several researches like Menopause-Specific QOL (MENQOL),10 t-test,14 χ2 test,15 etc. Through MENQOL (consisted with 22 factors) technique, all data was divided into four domains: vasomotor, psychological, physical and coherent disease. Vasomotor domain consisted with hot flashes, osteoporosis and sweating at night factors in while coherent disease domain consisted with type 2 diabetics, coherent heart disease factors. Psychological, physical domain factors is mentioned in Table 1. Chi-test (χ2) is used for calculating correlation among QOL factors for both cases participants. The frequency distribution in Table 1 is calculated using equation 1.

Results
Among all female participants the mean of age and BMI were 61.55 ± 10.7 and 24.33 ± 4.41 respectively. The mean length of time since menopause for all participants was 14.13 ± 11.17 years. Among all participants only 60.7% was involved in physical activity work out their job work and 39.3% was not directly or indirectly involved in physical exercise. An overview of all participants the result is showing in Table 2 that early menopausal female number is twice than late menopausal female number in Bangladeshi women. Table 2 shows for BMI that 56% participants in good level, 23.3% ongoing in bad level and 20.7% already reached in bad level. The research work has been done by two approaches like data mining approaches and statistical approaches.
Through data mining approach, Table 3 shows that feeling tried or lacking in energy & dizzy and depression are the most significant factors for both early and late menopausal women. It also shows that coherent heart disease and type 2 diabetics are the least significant factors for both early and late menopausal women perspective to Bangladesh. Osteoporosis holds the 3rd rank for late menopausal women in while feeling tense or nervous for early menopausal women. Osteoporosis factor has more impact on QOL of both early and late menopausal women than hot Flashes. But Table 3 shows that osteoporosis and hot flashes have high impact on QOL of late menopausal women than early menopausal women. Concentrating problem has holed 4th rank in both cases. Other factors ranking is mentioned in details on Table 3 that is designed using data mining technique. Finally Table 3 is showing that physical and disease factors have more impact on QOL of late menopausal women than early menopausal women but psychological factors have vice-versa impact.
Through Table 1, in vasomotor domain osteoporosis (around 72%) factor has highest impact on QOL of women for all cases and hot flashes (64%) has second highest place. Similarly in psychosocial domain depression (around 81.3%) holds first rank among all factors and feeling tense or nervous (around 76.7%) is in second rank. Feeling tried or lacking in energy and dizzy (around 82.7%) factor has most significant impact on QOL of both early and late menopausal women not only in physical domain but also among all domain. Early menopausal women have more heart beating rate than late menopausal women. Table 1 shows that early menopausal women have faced more physical problem than late menopausal women. It also shows that coherent disease (like type 2 diabetics, coherent heart disease) may have no correlation with menopausal status.
Discussion
The natural menopausal age has been examined in several Bangladesh studies215 as well as South Asian studies16 and compared to other regions of the world.17 The mean age of participants in this research was 61.55 ± 10.7 years and the mean menopausal time length was 14.13 ± 11.17 years. This is higher than studies down in several places in Bangladesh (51.14 years)15 and (53.31 years),2 in Singapore (50 years),16 in Nigeria (57.2 years).18 This research evaluated QOL of women in Bangladesh with menopausal symptoms on WEKA toolkit and MENQOL. MENQOL was using since 1996 with four domains: vasomotor, psychological, physical and sexual (but here used coherent disease). It has been applied in some developing countries1920 and also in Europe.21
In this study feeling tried (83%) is the highest significant factor among 25 factors for both early and late menopausal women in Bangladesh which is quite similar with the report of other place in Bangladesh2 and the study.22 African-American women reported23 that hot flashes is most frequent (45.6%) factor followed by Caucasians (31.2%), Hispanic (35.4%), Chinese (20.5%) and Japanese (17.6%). In our study hot flashes factor is 64% quite similar with the report.102425 But osteoporosis (72%) is more frequent than hot flashes in our study. Depression (81%) has the 2nd highest impact on QOL of Bangladeshi women what is conducted with the other report.26
Conclusions
The final result for all domains suggested that psychosocial, physical and vasomotor menopausal symptoms are strongly associated with QOL for both early and late menopausal women respectively. But coherent disease domain is less correlated with QOL. This research also describes that the early menopausal women have to face more problem of menopausal symptoms than late menopausal women in Bangladesh.
Limitations
As a cross sectional studies it have some limitations. All data was collected through face to face interview using Bengali questions what might be contained wrong information for participant's mistake. A few among of data was collected from 3 different places. The frequency of menopausal symptoms might be changed for large amount of data for more places.


 XML Download
XML Download