

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Flexible endoscopes are essential instruments for the diagnosis and treatment of many digestive disorders. They have very complex structures made up of fibrotic bundles and multiple long narrow tubular channels. Endoscopes are connected to an air and water system and a suction system. Furthermore, because endoscopes are reusable, there have been many concerns about their transmission of pathogens.1
In a comprehensive review article, 281 cases of pathogen transmission via gastrointestinal (GI) endoscopes were recorded to have occurred from 1966 to 1992. Of these, 253 cases predated the adoption of endoscopic society guidelines established in 1988,2 and only 35 cases of infection transmission have been reported over the 10 years following 1993.3 Improper cleaning and disinfection procedures were responsible for the majority of infection transmissions.23
Improper endoscope reprocessing, damaged endoscopes, contaminated automated endoscope reprocessors (AERs), and the complex structure of endoscopes can all threaten the safety of patients undergoing endoscopy. Therefore, endoscopic societies have established guidelines for the proper reprocessing of endoscopes. Most guidelines recommend multiple steps consisting of precleaning, cleaning, disinfection, rinsing, drying, and storage.45 Because endoscopes are categorized as semi-critical devices according to the Spaulding classification system, high-level disinfection (HLD) for reprocessing is needed.67 Because of the enforcement of proper endoscope reprocessing, the risk of microbial transmission has been greatly reduced.
In 2013, New Delhi metallo-β-lactamase-producing Escherichia coli and Klebsiella pneumoniae carbapenemase-producing K. pneumoniae were obtained by culture from the elevator channel of the endoscopic retrograde cholangiopancreatography (ERCP) endoscope. Although manual cleaning and HLD had been performed in accordance with the guidelines, these infections nevertheless occured.8 Lapses in proper endoscope reprocessing therefore still threaten the safety of patients.
In this respect, improved quality control systems would reduce patient safety concerns and substantially prevent infections from endoscopy. As part of the quality control of endoscope reprocessing, microbiological monitoring of endoscopes and their related facilities after HLD is being recommended by many organizations, such as the American Society for Gastrointestinal Endoscopy, the European Society of Gastrointestinal Endoscopy (ESGE), the European Society of Gastroenterology and Endoscopy Nurses and Associates (ESGENA) committee, and the Gastroenterological Society of Australia (GESA).4910
MICROBIOLOGICAL SURVEILLANCE: CULTURE AND NON-CULTURE METHODS
Microbiological surveillance methods can be classified into two kinds: microbial culture and non-culture methods. Non-culture methods consist of bioburden assays, adenosine triphosphate (ATP) bioluminescence, and quantitative polymerase chain reactions (PCRs).
Microbial culture
The majority of organizations recommend microbial cultures for monitoring. The ESGE recommends that surveillance cultures be assessed at intervals of not more than 3 months. Moreover, the maximal total microbiological count should be <20 colony-forming units (cfu) for fluid collected after flushing the endoscope channels with 20 mL of sterile saline solution, with placement of 1 mL of the fluid on each agar plate.9 However, the accessibility to microbiology laboratories and the relative slow turnaround time make this method impractical,11 and standard culture methods cannot isolate viruses.4 Nevertheless, surveillance culturing to monitor endoscopes after reprocessing has been widely accepted because of its simple methodology and cost effectiveness, as well as the large number of accumulated studies supporting its use.121314
Bioburden assays
Bioburden assays detect proteins on the surface of endoscopes; protein and blood materials within the biopsy channel of endoscopes; and proteins, blood, and carbohydrates residing within the channel of endoscopes.911 These assays are easy to use and can produce rapid results. Furthermore, several commercial test kits are available, such as Scope-Check (Valisafe America, Tampa, FL, USA) and EndoCheck and ChannelCheck (Health Mark Industries, Fraser, MI, USA). Surface sampling with swabs, channel sampling with swabs, and sterile water flushing are conducted, and the swab or water sample is then mixed with the test reagent. It takes 10 to 90 seconds for results to be obtained. The proposed criteria for organic and bioburden residues remaining after proper manual cleaning and before HLD include <6.4 mg/cm2 of protein, <1.2 mg/cm2 of carbohydrate, and <2.2 mg/cm2 of hemoglobin.15
Adenosine triphosphate bioluminescence
Because ATP is present in microorganisms and cells, this test enables estimation of the contamination condition after reprocessing. The technique uses the light-producing reaction between ATP, luciferin, and luciferase to estimate the levels of ATP in a sample. The results can be obtained within a few minutes. Luminometers convert the number of photons released in the reaction into relative light units (RLUs). The proposed criterion is achieved when the bioluminescence reading is <200 RLUs.16 The sensitivity is 0.46 to 0.75 and the specificity is 0.43 to 0.81, compared with routine microbiological culturing. Although it does not seem appropriate to replace routine microbiological culturing with the ATP bioluminescence assay,17 ATP bioluminescence can provide a rapid and reliable measure of the effectiveness of the cleaning step prior to terminal disinfection.1819 The Centers for Disease Control and Prevention (CDC) protocol comments that non-culture methods such as ATP bioluminescence need systemic validation owing to a lack of consistent correlation to bacterial concentrations.20
Polymerase chain reaction
PCRs have been used for detecting the human immunodeficiency virus, hepatitis B virus, hepatitis C virus, and Helicobacter pylori. Even if the test result is positive; however, it does not necessarily mean a presence of infectivity.212223 As part of the new non-culture-based methods, measurement or quantitative PCR for monitoring needs to be further optimized because of its low specificity.24
MICROBIOLOGICAL MONITORING BY MULTIPLE ORGANIZATIONS/INVESTIGATORS
Many organizations and investigators recommend microbiological surveillance of endoscopes, but some do not. The French Gastroenterology Society,25 ESGE-ESGENA,9 the GESA and the Gastroenterological Nurses College of Australia (GESA-GENCA), and the New Zealand Standards Expert Committee (SNZ HB) recommend microbiological surveillance testing of endoscopes after reprocessing in their guidelines. Although guidelines in the USA do not recommend routine culturing, the CDC has introduced the surveillance culture methods of other international guidelines.20 Moreover, there are some disparities among the guidelines for microbiological monitoring, in that the surveillance frequency, sampling methods, and sampling sites are different.
Surveillance frequency
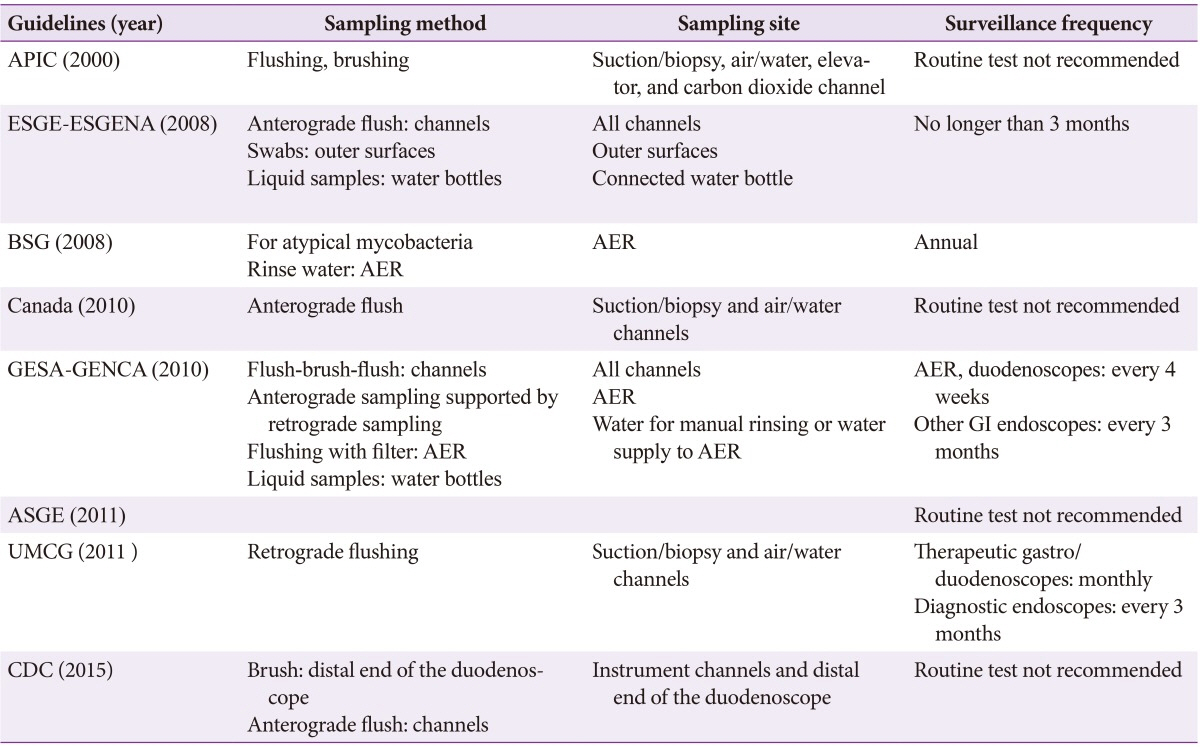
The GESA recommends microbiological surveillance every 4 weeks on AERs and duodenoscopes and every 3 months on other GI endoscopes. The ESGE-ESGENA guideline committee recommends the intervals to be no longer than 3 months. The British Society of Gastroenterology (BSG) guidelines recommend annual surveillance testing.
Sampling methods and sites
Sampling from the channel of the endoscope can be performed in an anterograde or retrograde manner. Anterograde sampling refers to collection of the last-rinse water at the distal end of the endoscope. Retrograde sampling refers to collection of the water that is flushed from the distal end to the proximal end. Because retrograde sampling is considered more sensitive than anterograde sampling, the former is recommended for monitoring endoscopes after reprocessing.2426 Flushing or flush-brush-flush methods for sampling of the internal channel are introduced in some studies and guidelines.
Table 1 shows the sampling methods and sites and frequency of microbiological surveillance culturing set by different guidelines.
Surveillance culture target
It is hard to test routinely for all species of bacteria, fungi, and viruses, so a culture target has to take into account the objective and cost. The BSG guidelines recommend annual testing for atypical mycobacteria in AERs. In the ESGE-ESGENA guidelines, Enterobacteriaceae, Pseudomonas aeruginosa, and staphylococci should be tested as indicator organisms, and atypical mycobacteria culture is recommended. The GESA-GENCA guidelines do not recommend routine testing for Legionella spp., anaerobes, H. pylori, and viruses. They recommend that bacterial cultures be directed to the detection of oral and enteric microorganisms such as coliforms (including Salmonella), enterococci, and viridans streptococci (but not anaerobes), as well as non-fermentative gram-negative bacilli (including Pseudomonas spp.). In samples from automated processors, non-fermentative gram-negative bacilli (including Pseudomonas spp.) and rapid-growing mycobacteria are the targets.
In the University Medical Center Groningen guidelines, bacterial isolates and yeasts are identified according to standard determination schemes.27
Culture results and interpretation
It is important to know how to interpret the culture results and what to do with the results. In the BSG guidelines, the presence of skin and environmental contaminants is not interpreted as a failure of disinfection. It simply means that endoscopes are not handled in a sterile fashion after decontamination. In the ESGE-ESGENA guidelines, growth of Enterobacteriaceae means insufficient cleaning and/or disinfection procedures, whereas growth of P. aeruginosa implies insufficient final rinsing and/or insufficient drying of endoscopes before storage. Growth of staphylococci results from endoscope recontamination. In the case of atypical mycobacteria (Legionella organisms) growth, contamination of the washer-disinfector and water system is suspected. For channels, the total microbiological count should be <20 cfu/channel; for water samples, it should be <10 cfu/100 mL. According to GESA-GENCA indications, growth of low numbers of skin microorganisms means contamination during the collection process rather than a significant problem with the disinfection or cleaning process, whereas growth of Pseudomonas spp. or other non-fermentative gram-negative bacilli is cause for serious and immediate concern and response. The repeated growth of significant numbers of enteric microorganisms from one instrument implies a mechanical defect in that instrument. Significant numbers of enteric microorganisms from a variety of instruments are most likely a result of inadequate reprocessing. The isolation of any Salmonella or Shigella species is a cause for concern.
CONCLUSIONS
Endoscopy-related infections can cause serious morbidity and therefore require attention from both patients and physicians. The need to obey every step of endoscope reprocessing meticulously cannot be over-emphasized. The majority of endoscopy-related infections are preventable with precise and careful endoscope reprocessing. However, factors such as endoscope damage, faulty AERs, and biofilms inside the endoscopic channels are attributable to endoscopy-related infections despite of meticulous reprocessing. Therefore, microbial monitoring is important. Unfortunately, all guidelines are inconsistent concerning the frequency and method of the microbiological monitoring. Although daily or per procedure real-time monitoring is ideal, this is currently not possible. Individual institutions should establish their own guidelines for microbiological monitoring, taking into consideration institutional cost and environmental factors.
 XML Download
XML Download