

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Fibrovascular polyps (FVPs) of the esophagus are rare, benign intraluminal tumor-like lesions arising from the submucosal layer of the cervical esophagus.1 These masses are composed of loose or dense fibrous tissue, vascular structures, and adipose tissue covered by normal squamous epithelium.2 FVPs are the most common intraluminal, nonepithelial neoplasms of the esophagus, accounting for 0.5% to 1% of all benign esophageal tumors.3 They are most typically observed in middle-aged and elderly men.4 Because of an initial lack of symptoms, the tumor attains a very large size inside the lumen of the esophagus.5 Thus, FVPs may cause dysphagia and sudden death from asphyxiation when the polyp regurgitates and occludes the larynx.6 In the present report, we describe the case of a patient with an FVP who suffered from snoring and asphyxia during sleep. This individual was successfully treated endoscopically.
CASE REPORT
A 51-year-old man visited our institution for routine endoscopy. He had a long history of snoring and obstructive sleep apnea. His wife frequently heard his labored breathing while he slept and would wake him up. However, the patient did not undergo a complete medical examination because he regarded his condition as simple snoring. Moreover, he did not have a history of regurgitation, pain during swallowing, weight loss, or signs and symptoms of upper gastrointestinal bleeding. His medical and surgical history was unremarkable, and the physical examination findings were normal. Laboratory results were also unremarkable.
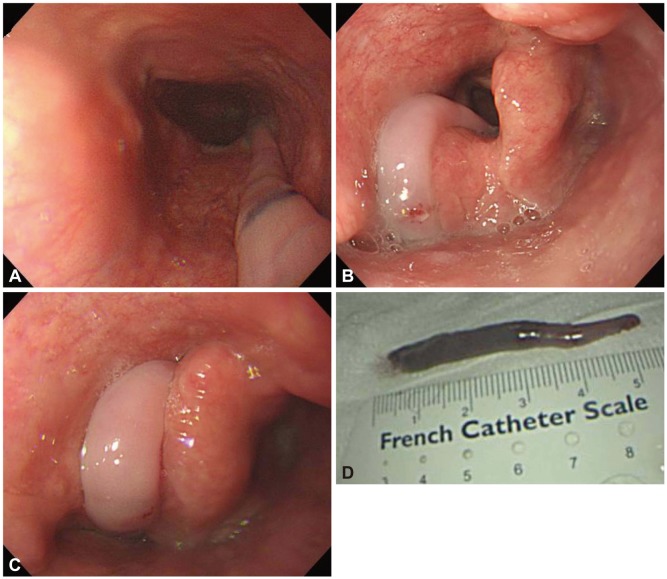
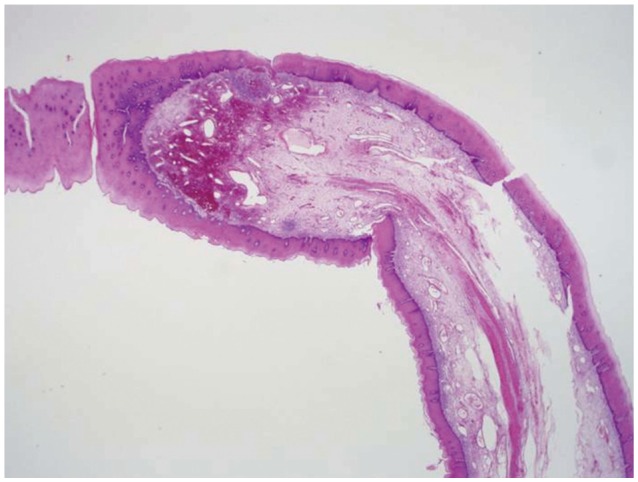
Endoscopy revealed a pedunculated polyp, >5 cm in length, that was detected immediately after inserting the endoscope into the patient's throat (Fig. 1A). The polyp arose from just below the pyriform sinus and regurgitated into the oral cavity during endoscopy. Occasionally, the polyp passed through the vocal cords (Fig. 1B) and obstructed the airway (Fig. 1C). We removed the polyp endoscopically using a polypectomy snare (Fig. 1D) because we believed that the polyp could induce asphyxia during sleep. Histopathological examination indicated that the polypoid lesion contained vascularized loose fibrous shafts covered by squamous epithelium with acanthosis, which were indicative of an FVP (Fig. 2). The patient was discharged on the next day without any complications. At the 3-month follow-up examination, the patient was found to be doing well without any further occurrence of snoring or sleep disturbances.
DISCUSSION
FVPs usually remain asymptomatic for years until reaching significant and occasionally enormous sizes because of their slow growth. The most frequently reported symptoms of FVPs are progressive dysphagia and the sensation of a mass. The severity of these symptoms is reported to be related to increases in polyp size.7 The other complaints include retrosternal or epigastric discomfort, odynophagia, vomiting, bleeding, weight loss, and respiratory symptoms such as persisting cough or difficulty in breathing.8
Because they originate from the cervical esophagus and due to their loose, elongated features, FVPs easily regurgitate into the mouth or pharynx. However, although asphyxia due to a regurgitating FVP is well known, no endoscopic imaging evidence indicating that regurgitating FVPs can be aspirated into the airway and cause asphyxia is available. In the present case, we obtained high quality pictures of the regurgitating polyp that was obstructing the airway during endoscopy. In addition, we observed that the patient suffered from breathing difficulties and coughing when the FVP passed through his airway.
Similar to the present case, relatively small regurgitating FVPs induce snoring and sleep disturbances. However, extremely large FVPs can cause potentially life-threatening conditions if the regurgitating polyps completely obstruct the airway.9 Due to the rarity of FVPs in the esophagus, there are no data on the mortality rate due to FVP-associated asphyxia. However, there have been seven reported cases of death due to aspiration of regurgitating polyps,7 and up to 30% of patients may die without a correct diagnosis.10 Therefore, FVPs of the upper esophagus should be removed regardless of the symptoms.
The definitive treatment of an FVP is excision, which can be performed either endoscopically or surgically. Appropriate treatment depends on the accurate assessment of the origin, diameter, and vascularity of the pedicle along with tumor size.11 Giant polyps or ones with a thick and richly vascularized pedicle are removed by surgical excision, which enables controlling of the bleeding.12 The pedicle should be completely excised because incomplete excision may result in recurrence.13 Endoscopic resection is also an option but is not preferable for treating giant FVPs because of the risk of hemorrhage from vessels in the polyp stalk. In general, endoscopic resection is recommended for polyps less than 2 cm in diameter and with a thin pedicle.14 Endoscopic ultrasonography can be helpful for identifying the presence of feeding vessels prior to attempting endoscopic resection.15 In the present case, we successfully removed the FVP endoscopically, even though it was more than 5 cm in length, because the pedicle was relatively thin. No complications, such as bleeding or recurrence, occurred during the 3 months after endoscopic resection.
In summary, FVPs of the esophagus are benign tumors. Despite their slow growth, these lesions should be removed because of potentially serious complications such as asphyxia or sudden death. Appropriate treatment should be based on FVP size and origin as well as on vascularity of the pedicle.
 XML Download
XML Download