

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Afferent loop obstruction is a potentially life-threatening complication of Billroth II gastrectomy or Roux-en-Y hepaticojejunostomy (RYHJ). Afferent loop syndrome caused by an enterolith is rare.1 Formation of the enterolith is presumed to be related to hypomotility or stasis of the bowel that is altered anatomically after Billroth II subtotal gastrectomy.
When the enterolith obstructs the lumen of the afferent limb, the intraluminal pressure of the intrahepatic duct (IHD) and proximal jejunal limb may be elevated, and bacterial overgrowth in the lumen of an obstructed bowel may cause ascending bacterial infection of the biliary tree. Few cases of afferent loop obstruction caused by an enterolith have been reported. Most cases are treated with surgery for removal of the enterolith because the afferent loop of the jejunum is long and tortuous and endoscopic access to the enterolith is difficult.2-7 Here, we report a case of afferent loop syndrome with acute cholangitis caused by an enterolith that was treated with a percutaneous transhepatic cholangioscopic procedure.
CASE REPORT
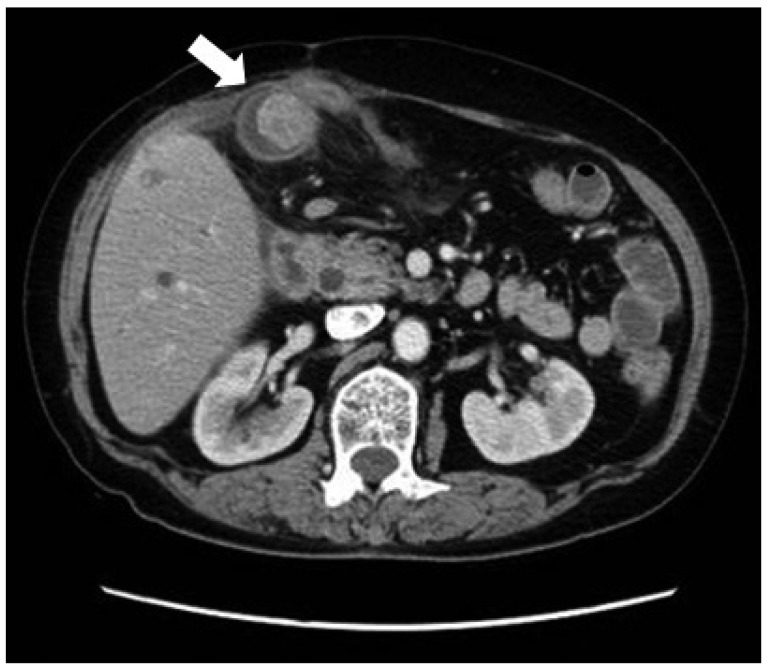
A 74-year-old woman was admitted with a 2-day history of fever and acute abdominal pain. The patient had undergone choledochal cyst excision, left hepatectomy, and RYHJ for IHD stones and a choledochal cyst 12 years previously. On admission, blood pressure was 90/57 mm Hg, pulse rate was 116 beats per minute, temperature was 38.5℃, and tenderness in the right upper quadrant of the abdomen was detected. Laboratory findings were as follows: white blood cell count, 14,900/mm3 (normal range, 4,000 to 10,800); platelet cell count, 81,000/mm3 (normal range, 150,000 to 400,000); C-reactive protein, 11 mg/dL (normal range, 0 to 0.3); aspartate aminotransferase, 129 IU/L (normal range, 7 to 38); alanine aminotransferase, 187 IU/L (normal range, 4 to 43); total bilirubin, 6.2 mg/dL (normal range, 0.1 to 1.3); and alkaline phosphatase, 432 IU/L (normal range, 103 to 335). An abdominal computed tomography (CT) scan showed a single stone in the sixth branch of the right IHD and a stone measuring 3 cm in the afferent loop with diffuse dilatation of the upstream small bowel loop and IHD (Fig. 1). Afferent loop syndrome caused by an enterolith was diagnosed on the basis of the clinical features and imaging studies.
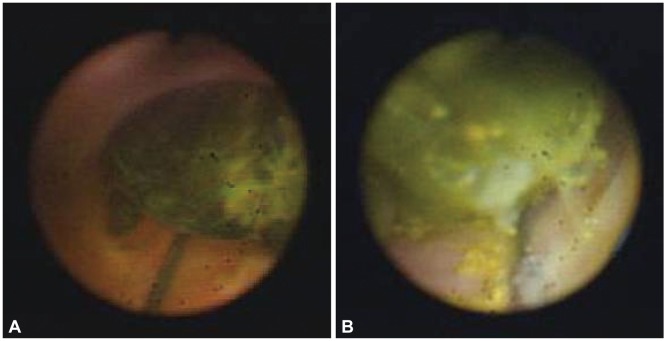
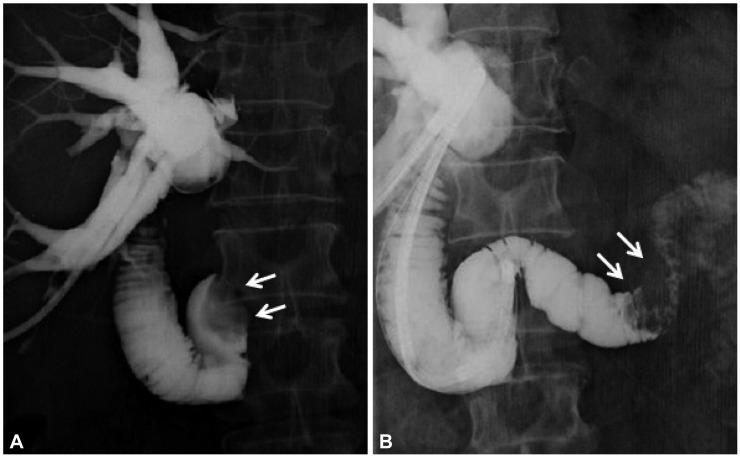
Because the patient was septic and her condition was unstable, we performed urgent percutaneous transhepatic biliary drainage (PTBD). A 10 Fr pigtail catheter for PTBD was passed over the guide wire and placed in the jejunal limb through B6 after B6 of the IHD was punctured using a 21-gauge hollow needle under ultrasound guidance, and a guide wire was inserted through the needle into the bile duct. After PTBD, the patient showed a gradual improvement of her general condition. Because the enterolith was located in the jejunal limb near the hepaticojejunostomy site on abdominal CT and cholangioenterogram, peroral endoscopic access to the enterolith was difficult, and surgical treatment was refused by the patient, we decided to perform percutaneous transhepatic cholangioscopy (PTCS) for removal of the IHD stone and the enterolith. First, the PTBD tract was dilated to 18 Fr using a dilator to allow insertion of a standard choledochoscope (CHFP20Q; Olympus Co., Tokyo, Japan) into the bile duct 7 days after PTBD. One week later, PTCS was performed for stone removal. Cholangioscopic examination showed an IHD stone and a large enterolith. The IHD stone was a black-pigmented stone and the jejunal loop stone was grayish and hard (Fig. 2). Because the hepaticojejunostomy site was not stenotic and an enterolith was located in the jejunal limb near the hepaticojejunostomy site, the cholangioscope could access the enterolith. Electrohydraulic lithotripsy (EHL) was performed to fragment the enterolith. An electrohydraulic shock wave generator (Lithotron EL 25; Walz-electronic Inc., Rohrdorf, Germany) set at an output of 2,000 V was used for the generation of shock waves of increasing frequency (intensity of 500 mJ), which were applied with a continuous sequence of discharge. After stone fragmentation, the enterolith was pushed out through the jejunojejunal anastomosis to the efferent loop using the cholangioscope and a saline flush (Fig. 3). The cholangiogram showed that the IHD and the afferent loop were clear, without any remnant stone. The PTBD catheter was removed, and the patient began oral intake 1 day after the procedure. The patient made a full recovery without any complications, and was discharged 2 days after the procedure.
DISCUSSION
Afferent loop obstruction is an unusual but potentially life-threatening complication of Billroth II gastrectomy or RYHJ. Possible causes of the obstruction include mechanical obstruction of the afferent limb caused by adhesions, internal hernias, volvulus, intussusception, intestinal kinks/strictures, malignancy, and rarely, an incarcerated enterolith.1 The etiology of enterolith formation in the afferent limb includes limb dysmotility and bacterial overgrowth, and the cause of limb dysmotility is the vagal denervation or proximal disconnection of the afferent limb from the main pacemaker in the duodenum.2
In such cases, surgery has been the treatment of choice for enterolith removal because nonsurgical removal through the peroral or percutaneous route is difficult technically.3-7 Successful endoscopic removal of the enterolith in the afferent loop is rare.7 However, theoretically, endoscopic treatment through the percutaneous route should be possible for removal of an enterolith from the afferent loop in special cases such as an enterolith located proximal to the hepaticojejunostomy site or through the use of balloon enteroscopy. PTCS with EHL is a low-risk procedure for removal of the enterolith after PTBD. In the absence of complications 1 day after the procedure, the PTBD catheter can be removed and patients can resume oral nutrition.
In the present case, we first created a PTBD tract for retrieval of the IHD stone. After removal of the IHD stone, we attempted to access the enterolith in the afferent loop through the PTBD tract and hepaticojejunostomy using the cholangioscope. We could approach the enterolith in the afferent loop because it was located in the jejunal limb adjacent to the hepaticojejunostomy site.
Because of the risk of afferent loop syndrome caused by enterolith recurrence in the present case, regular clinical follow-up examinations are recommended for such cases in the future. In addition, the use of prokinetic agents or restrictions in the administration of proton-pump inhibitors should be considered in such cases.
In conclusion, PTCS with EHL may be a treatment option for afferent loop syndrome caused by an enterolith in patients who underwent RYHJ.
 XML Download
XML Download