

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In gastrointestinal (GI) bleeding, endoscopic diagnosis and therapy is the initial treatment of choice as it is imperative to determine whether bleeding is variceal or arterial, and endoscopic treatments usually achieve primary hemostasis in the majority of patients. However, 10% to 30% of these patients have repeat bleeding.1 In a recent national audit in the UK, salvage surgery and transcatheter arterial embolization (TAE) were required in fewer than 4% of patients with nonvariceal upper GI bleeding.2
After the first report of selective TAE of gastroepiploic artery for the control of acute gastric bleeding,3 improvements in interventional devices and embolic materials and wider availability of skilled interventional radiologists have increased the utility of TAE procedures in the management of GI bleeding.4 TAE seems now accepted as the salvage treatment of choice over surgery for acute bleeding in the upper GI tract despite endoscopic treatment. Decision making to choose TAE or surgery depends on the condition of the patients or their availability.
INDICATIONS/CONTRAINDICATIONS
Indications
A typical candidate patient presents with the followings: 1) endoscopy-refractory acute GI bleeding. In previous studies, endoscopy had been performed and failed in average 99% of the study patients: significant amount of blood in the stomach, large ulcer size, location of lesion at posterior bulbar duodenum, multiple lesions, and lesser curve were identified as causes of endoscopic failure.5 High risk patients tend to be directed toward TAE rather than surgery;5 2) massive bleeding (transfusion requirement of at least 4 U of blood over 24 hours) or hemodynamic compromise (systolic blood pressure <100 mm Hg and heart rate >100 beats per minute or clinical shock); and 3) recurrent bleeding after surgery.
It is important to do the angiography while the patient is bleeding. It is not necessary to wait until the patient is hypotensive or unstable.
Contraindications
There are no absolute contraindications because angiography and TAE may be needed as lifesaving procedures. Relative contraindications include renal insufficiency, contrast allergy, and uncorrectable coagulopathy. There is increased risk of gastric or duodenal infarction after TAE in patients with previous extensive upper GI surgery or radiotherapy. If the rate of bleeding is massive, surgery may be preferable to angiography, since angiography may not be able to control the bleeding as quickly as surgery.4
TECHNIQUES OF ANGIOGRAPHY AND TAE
General rules
Digital subtraction angiography seems to have equivalent detection rate to scintigraphic images.4 The major limitation of angiography relates to the intermittent nature of bleeding, which can result in a negative result if the bleeding has temporarily stopped at the time of contrast injection.4
It is important to select a vessel that is most likely to supply the bleeding according to history, clinical signs, as well as localization provided by endoscopy, scintigraphic images or computed tomography scans. Thus, we can initiate treatment and stabilize the patient quickly. Aortograms are usually not performed, since only small percentage of contrast will get to the bleeding site and fill multiple overlapping vessels, making identification of the bleeding vessel difficult.
For upper GI bleeding, angiography is centered on the anatomy of the celiac artery; left gastric artery supplies superior lesser curvature and cardiac region, right gastric artery supplies inferior lesser curvature, short gastric artery from splenic artery supplies superior greater curvature and the fundus, and gastroduodenal artery supplies remainder of the stomach and duodenum. The superior mesenteric artery may supply portions of the duodenum, mostly by way of pancreaticoduodenal anastomoses, which are important as a rich collateral supply, but it also may be responsible for rebleeding after TAE.
For lower GI bleeding, angiography is centered on the superior and inferior mesenteric arteries; superior mesenteric artery supplies portions of the duodenum to transverse colon, and inferior mesenteric artery supplies the descending colon, sigmoid colon to superior portion of the rectum. When rectal bleeding is suspicious, both internal iliac arteries should be included because middle and inferior rectal branches come off internal iliac arteries.
Methods to enhance bleeding detection
1) Glucagon and Buscopan may be given before the procedure to decrease bowel motility and motion artifacts during digital subtraction angiography.
2) Provocative angiography such as infusion of tolazoline (vasodilator), heparin, or even thrombolytics (tissue plasminogen activator), can stimulate bleeding.
3) Longer injection durations or use of carbon dioxide for contrast medium can also improve sensitivity for small bleedings.5
4) Endoscopic clips placed around the area of bleeding during pre-embolization endoscopy can help localize the accurate bleeding vessels. If no extravasation is seen despite the injection of contrast, then the branches terminating at the clip are superselected using microcatheter techniques and embolized.6,7
5) Oblique views can provide clearer view of colic vessels in flexures. Right and left anterior oblique views open up hepatic and splenic flexures, respectively.
Angiographic findings and TAE
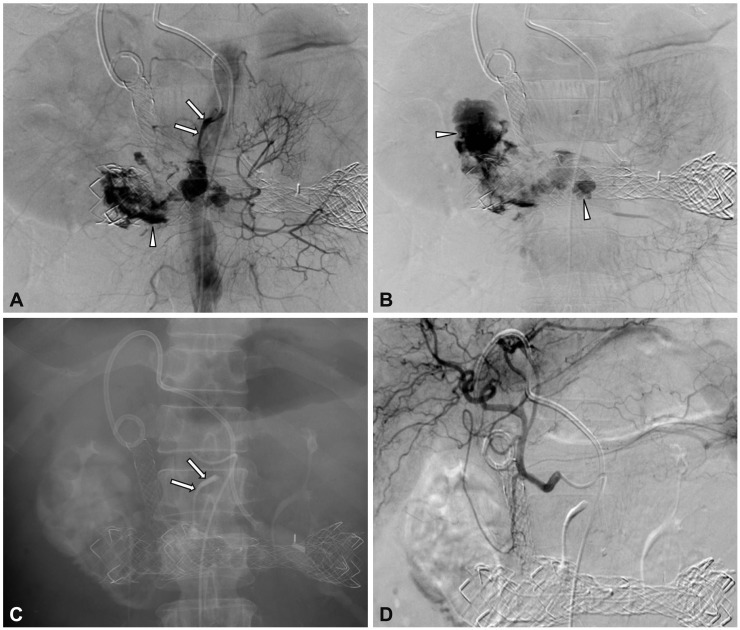
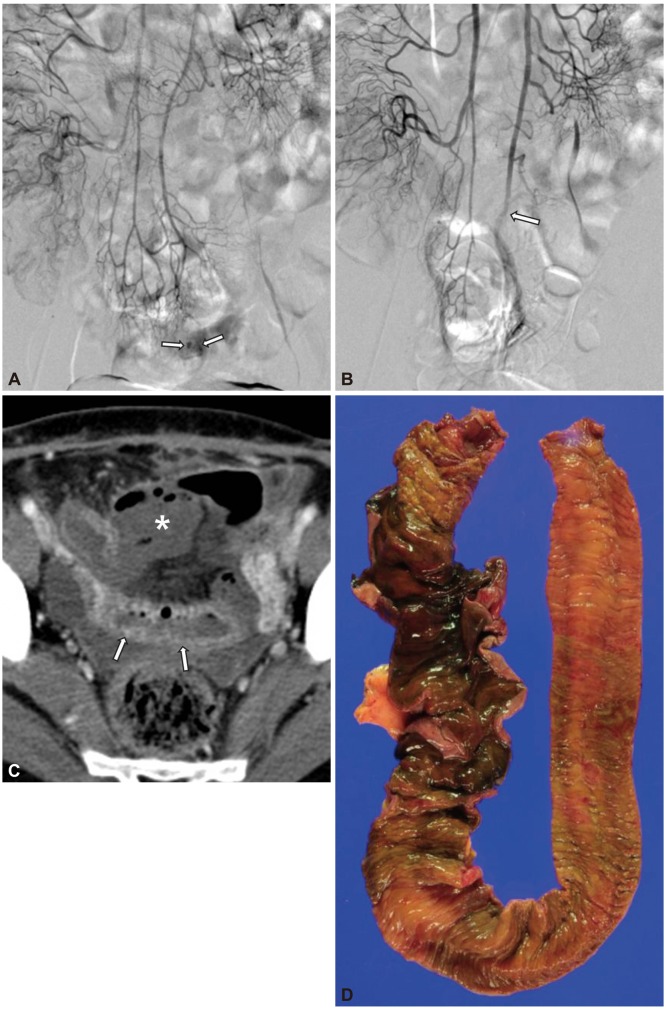
The only direct angiographic sign of GI bleeding is extravasation of contrast medium into the bowel lumen (Fig. 1). Indirect signs include aneurysms/pseudoaneurysms, vessel irregularity, vessel cutoff and arteriovenous/arterioportal shunting, neovascularity, and increased vascularity from dilated arterioles (as seen in angiodysplasia) (Fig. 2).4
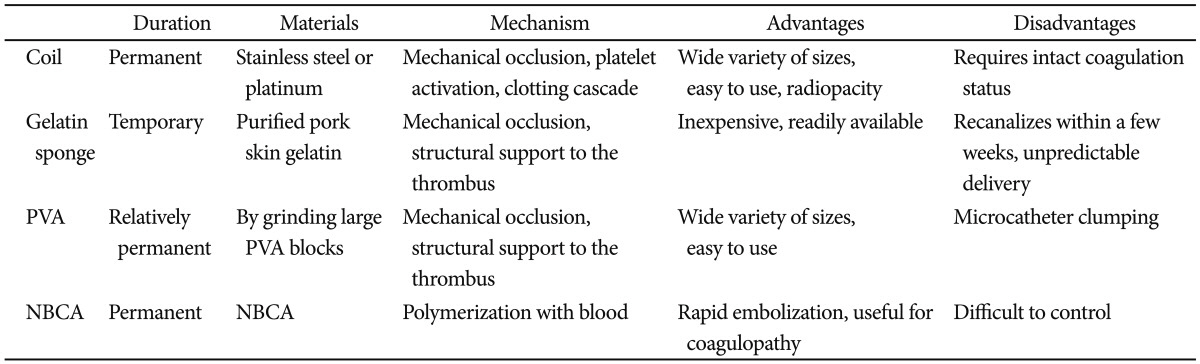
The choice of embolic agent depends on a combination of the vascular anatomy, angiographic findings, the achievable catheter position, and the operator's preference (Table 1). Vessel diameter and the nature of permanent or temporary embolization should be also considered. The most common embolic agents are metallic coils and gelfoam.8 Use of coils as the only embolic agent is significantly associated with early rebleeding, compared with the use of polyvinyl alcohol or gelatin sponge with coils.9,10 Use of N-butyl cyanoacrylate (NBCA) has gained acceptance recently (Fig. 1). It is a liquid embolic material with nonradiopaque nature and, therefore, it should be mixed with lipiodol to provide radiopacity and to control the viscosity. The more diluted NBCA concentration is, the deeper penetration to the distal is achieved. Usually NBCA: lipiodol ratio ranges from 1:1 to 1:4. It is advantageous for massive bleeding that requires urgent hemostasis, especially in patients with coagulopathy because of rapid polymerization with blood.
The tip of the microcatheter should be as distal as possible until the bleeding point (e.g., vasa recta in small and inferior mesenteric arteries). The distal location lowers blood pressure and facilitates clot formation, and risk of back flow to the bleeding point becomes lower. For example, in cases of small bowel branches, there is potential collateral supply when the microcatheter tip is in proximal arc. The best location of the microcatheter tip is vasa recta.
OUTCOMES
Summary of previous results
Five recent representative studies of TAE for nonvariceal GI bleeding in 228 patients showed technical success rates of 92% to 100% and clinical success rates of 51% to 83%.9,11-14 Inability to catheterize the bleeding branch as a result of difficult anatomy (e.g., tortuous hepatic artery) and occluded access (e.g., stenosed celiac trunk or common hepatic artery) were the most common reported cause of technical failure.8
Rebleeding rates were 9% to 47%, rates for surgery were 0% to 35%, and 30-day mortality rates were 3% to 27%. Such wide ranges in clinical success and rebleeding rates, rates for surgery, as well as 30-day mortality rates seem to have originated from different etiologies and clinical severities.
Is empiric embolization necessary?
Because of the intermittent nature of many incidents of GI bleeding, the incidence of a normal angiogram in patients with acute upper and lower GI bleeding was 52% (75 out of 143 patients) in one recent report.15 In the latter study, the incidence of angiographically negative outcome was significantly higher in patients with a stable hemodynamic status, or in patients with lower GI bleeding.
If no evidence of bleeding is found on pre-TAE arteriogram, then empiric embolization (usually with gelatin sponge and/or coils), defined as embolization without angiographic evidence of active bleeding, could be an alternative and is typically guided by endoscopic information regarding the location of the bleeding vessel.5 Empiric embolization for the upper GI bleeding is advocated because GI bleeding is quite intermittent and accompanied by high rebleeding and mortality rate, if untreated. Angiographic confirmation of a bleeding site seems not a prerequisite for TAE in the upper GI bleeding. Several studies showed no difference in clinical outcomes between patients with negative and patients with positive angiography results when both were treated with TAE.14,16-19
TAE versus surgery
The wide array of alternatives for the treatment of GI bleeding after endoscopic failure make the decision of when to resort to emergency surgery more difficult, especially in patients with high surgical risk.5
Controlled trials comparing TAE with surgery as a salvage procedure for failed endoscopic therapy is limited. Two retrospective comparative studies involving a total of 70 and 91 patients, showed at least similar efficacy in terms of the rate of rebleeding, morbidity, and mortality.20,21 Whereas, a recent retrospective comparative study including 93 patients showed significantly higher rebleeding rates in patients after TAE compared with surgery (46.7% vs. 12.7%), although the authors admitted that only coil or gelfoam use in the earlier cases could have contributed to the high rebleeding rates in TAE group.22
Nonetheless, TAE could not replace surgery. Although continuous bleeding demands emergency TAE, especially in high surgical risk patients, surgery is preferred in young and healthy patients, especially with large and/or multiple peptic ulcers, in the absence of an evidence proving the inferiority of TAE in such a setting.
Complications
Periprocedural complications are related to underlying conditions such as advanced age or comorbidities. Many technical complications are without clinical consequences and mostly preventable.
TAE in the upper GI tract above the ligament of Treitz is generally considered very safe because of the rich collateral supply to the stomach and duodenum. However, the risk of significant ischemia or stricture could be increased when potential collateral vessels are damaged from previous upper abdominal surgery, radiotherapy, or severe atherosclerosis, when TAE extent is wide (Fig. 2), or when liquid agents such as NBCA, or very small particles advance far into the vascular bed.4
Lang23 reported a 16% (9/57 patients) incidence rate of duodenal strictures following TAE. If true bowel infarction occurs, surgical resection is generally required (Fig. 2). For more chronic ischemic complications such as bowel stricture, balloon dilation may be possible, but surgical resection should be considered if the stricture is resistant to balloon dilation.
 XML Download
XML Download