

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Any decision-making process in clinical medicine may be simplified in a series of sequential steps that cumulatively lead to a clinical diagnosis or intervention. Thus, the additional benefit of any step must be balanced with the associated exploitation of medical and economic resources. When limiting our focus to diagnostic process, the additional value of any subsequent test will depend on the absolute increase in accuracy as compared with what was achieved prior to the test.
Histological examination of colorectal lesions has been considered in the last decades as a critical step in the decision-making process, because of its contribution in differentiating between nonneoplastic and neoplastic lesions, and - among those neoplastic - between noninvasive and invasive lesions.1,2 The relevance of postpolypectomy histological examination has been intimately related with the lack of any alternative in characterizing polypoid or nonpolypoid lesions prior to the pathological examination itself.1,2 Despite histological characterization of colorectal polyps has been generally considered as a gold-standard, some pitfalls may be identified. First, not all the removed polyps are actually retrieved, resulting into a complete loss of information in 10% to 20% of cases.3 Secondly, a high interobserver variability in the diagnosis of the degree of dysplasia and villous component - i.e., the unfavourable features discriminating between advanced and nonadvanced neoplasia - has been shown.4 Third, the same differentiation between hyperplastic and adenomatous histotypes is not perfect, with adenomatous tissue hidden in the nonexamined part of the embedded specimen. Fourth, there is no general consensus on the clinical meaning of histological characterization with divergent recommendations according to different guidelines.5,6
The need of postpolypectomy histological examination causes a substantial exploitation of medical and economic resources. It may be estimated that roughly one in every two patients undergoing screening or diagnostic colonoscopy are diagnosed with at least one polyp, thus requiring postpolypectomy pathological examination.7,8 Secondly, the vast majority of these polyps are diminutive (≤5 mm) with a very low prevalence of advanced neoplasia, marginalizing the clinical impact of pathological examination.7-9 Third, the estimated cost of the pathological examination is of the same magnitude with that of colonoscopy, heavily affecting the cost of colonoscopy screening without adding an equivalent contribution to colonoscopy efficacy.10-12 Fourth, the need of a new visit for communicating the postpathological surveillance interval generates a substantial and avoidable loss of productivity for the society, especially when considering that roughly 60% of the United States population undertakes a screening colonoscopy every 10 years.13
In order to address these pitfalls, a policy of discarding the postpolypectomy pathological examination has been proposed, also named as predict-resect-and-discard policy.14-16 Its main assumption is that if endoscopy may predict in vivo the histotype of the polyp, the additional value of histological examination may be marginalized, becoming inefficient and/or cost-ineffective.10-12 Predict-resect-and-discard policy has been mainly prompted by the technical evolution of endoscopic imaging, leading to a new field defined as advanced endoscopic imaging, with the main aim of differentiating between hyperplastic and neoplastic, as well as between noninvasive and invasive neoplastic lesions.17,18 However, before implementing a predict-resect-and-discard policies, several issues need to be addressed. First, in vivo prediction of polyp histology is required to reach an adequate level of accuracy, in order to minimize the possible contribution of postpolypectomy histological examination to the decision-making process. Secondly, a high degree of inter and intraobserver agreement is required, in order to assure its reproducibility. Third, a feasible training and learning curve must be in place, in order to result into an adequate generalizability of the predict-resect-and-discard strategy. Fourth, advanced imaging techniques need to be supported by the available endoscopic systems. Fifth, the appropriateness of the clinical recommendations - i.e., the postpolypectomy surveillance intervals - should not be deteriorated by the exclusion of pathological examination. Sixth, a standardized and formal reporting of in vivo histological prediction must be in place, in order to prevent misuse or eventual medical litigations related with the implementation of this policy.
Aim of this review is to address the pros and cons of a predict-resect-and-discard policy based on the data available in the literature.
ADVANCED ENDOSCOPIC IMAGING
Standard white light endoscopy has been regarded as inaccurate to accurately predict in vivo the histological features of colorectal lesions. Sensitivity has been shown to broadly range between 60% and 90%, with specificity ranging between 40% and 90%.19-21 The evolution from standard to high-definition endoscopy disappointingly failed to meaningfully improve the suboptimal white light accuracy in characterizing colorectal polyps.19 The possibility to in vivo differentiate among different histotypes has been initially shown by Japanese endoscopists.2,17,18,22,23 Briefly, it was exploited the ability of some dyes - such as indigo carmine and methylene blue - to highlight the pit pattern of colorectal lesions at high-(optical) magnification endoscopy.2,17,18,22,23 The pit pattern of both polypoid and nonpolypoid lesions was shown to be intimately associated with the progressive distortion and elongation of colonic glands during colorectal cancer (CRC) carcinogenesis or, alternatively, with the evolution towards a serrated - mainly hyperplastic - histotypes.2,17,18,22,23 However, dye-chromoendoscopy failed to be successfully implemented in Western countries for several reasons. First, Japanese endoscopists appeared to be more prone to implement chromoendoscopy in colonoscopy, because chromoendoscopy had already been routinely adopted for population-based gastric cancer screening.24 Secondly, dye spraying has been generally discarded as time-consuming and inconvenient, also when considering the intensive volume of screening colonoscopies performed in Western countries.13 Thirdly, dye-chromoendoscopy requires a long-lasting learning curve, possibly including several hundreds of examinations.2,16,17,21,22 Fourth, chromoendoscopy has been pri-marily exploited for differentiating between endoscopically and surgically resectable submucosal cancer in nonpolypoid lesions rather than for discriminating between nonneoplastic and neoplastic lesions.2,16,17,21,22 Fifth, an excessive dye spraying may substantially reduce the visibility of the mucosa surrounding the targeted lesion, potentially affecting the detection rate of more serious lesions.
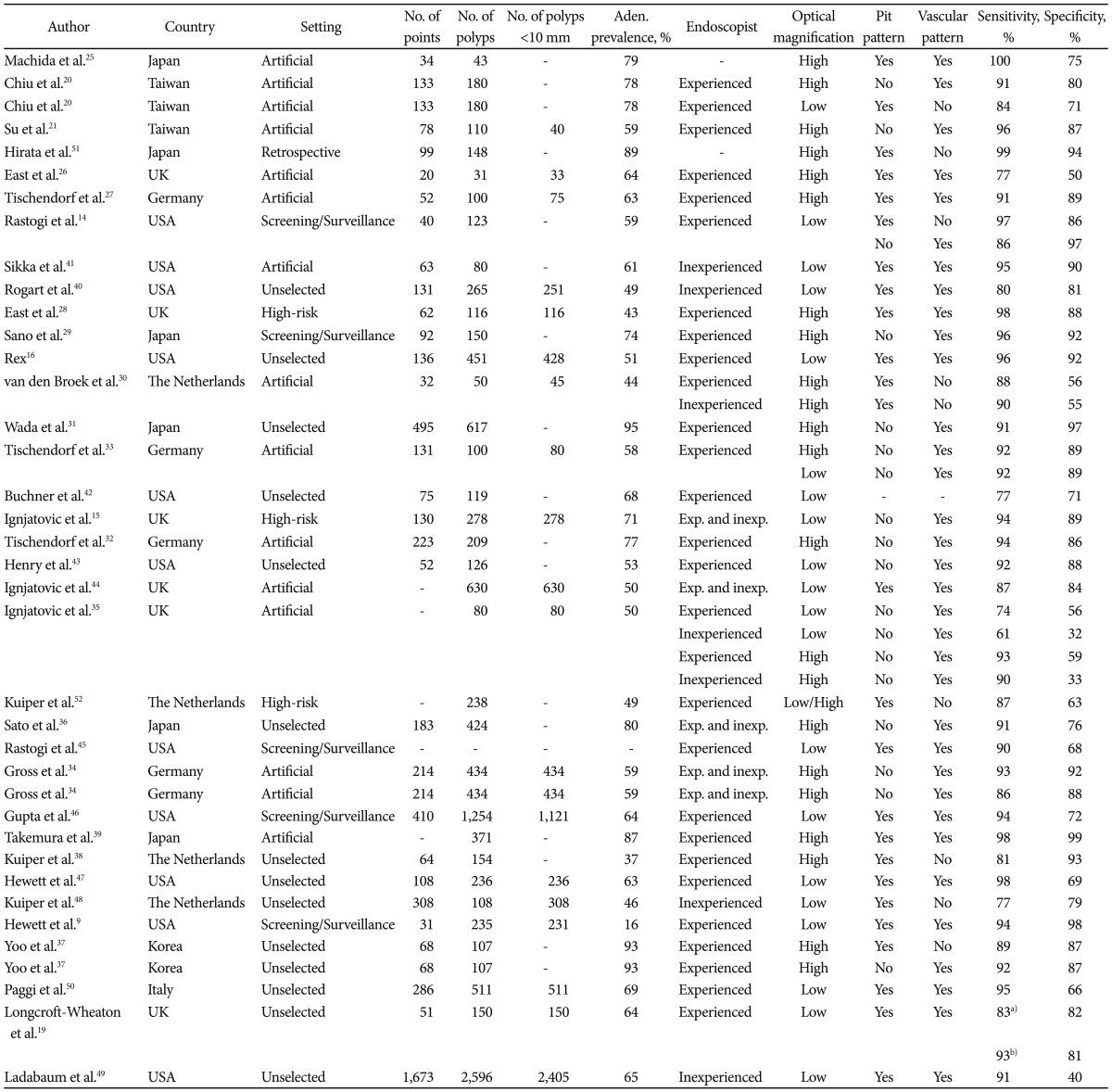
For all these reasons, there was the need of a major breakthrough to expand the success of advanced endoscopic imaging to Western countries. As detailed by Rastogi et al. in this issue of Clinical Endoscopy, the advent of electronic chromoendoscopy (EC) - such as narrow band imaging, Fuji intelligent color enhancement, and Pentax I-Scan - opened the door for the in vivo prediction of polyp histology in Western countries. First, EC has shown a promising accuracy in differentiating between adenomatous and hyperplastic polyps in several studies (Table 1),9,14-16,19-21,25-52 owing to the advantage of being extremely simple and fast to be activated. Secondly, the level of confidence of the operator in the in vivo prediction has been associated with EC accuracy, so that - by restricting the analysis only to the high-confidence diagnosis - EC accuracy may be further improved.9,15,16,47-49 Third, EC is available on the new generation of endoscopes, so that a widespread implementation of this technique may be expected. Fourth, a very fast and simple training and learning curve has been shown to be feasible, also leading to acceptable rates of inter and intraobserver agreements, thus assuring the generalizability and reproducibility of the in vivo characterization.25,47,53
PREDICT-RESECT-AND-DISCARD AND PREDICT-AND-DO-NOT RESECT POLICIES
The efficacy and safety of strategies based on in vivo characterization of colorectal lesions depends on a complex interaction between the accuracy values of EC, the expected prevalence of disease, and the types of surveillance intervals recommended. The main criticism to EC-based prediction is its inability in discriminating between nonadvanced and advanced neoplasia.9,14-16,19-21,25-50,54 Since unfavourable histological features - such as high-grade dysplasia or >20% villous component - predict a higher risk of metachronous advanced neoplasia,55 the identification of unfavourable histological features actually results into the assignment of a more intensive postpolypectomy surveillance (i.e., 3-years vs. -5/10-years).5,6 Therefore, EC-based policies should be implemented only when the risk of advanced neoplasia may be marginalized. When comparing the prescreening prevalence of advanced neoplasia - ranging between 4% and 10% - with that of subcentimetric polyps, such prevalence would appear to be marginal - i.e., ≤1% - in diminutive lesions, whilst ranging between 1% and 5% in 6 to 9 mm lesions.7,8,56 Consequently, the actual drawback of a predict-resect-and-discard policy for diminutive lesions would be the lack of characterization of one case of advanced neoplasia every ≥100 predictions, resulting into a 2/7-year delay in the postpolypectomy surveillance interval. Suggestively, the predict-resect-and-discard policy would still appear safer than the actual nonreferral policy implemented by computed tomography colonography and colon capsule, according to which diminutive lesions, irrespectively of whether (advanced) adenomatous or hyperplastic, should not even sent to post-test polypectomy.57,58 On the other hand, the application of EC-based policies to 6 to 9 mm lesions appears to be more controversial, because of the higher prevalence of advanced neoplasia within these lesions.7,46 However, the much lower prevalence of 6 to 9 mm as compared with ≤5 mm lesions in the general population would marginalize the impact of these lesions over the efficiency of EC-policies.8 The second criticism to in vivo prediction of polyp histology is the possibility of EC-false-negatives/positives results when discriminating between hyperplastic and adenomatous polyps (Table 1).9,14-16,19-21,25-52 This would result in the risk of either anticipating the postpolypectomy surveillance interval in those with an hyperplastic lesion misclassified at EC as adenomatous or delaying it in those with an EC-misclassified adenomatous lesion. The clinical consequences of EC-misclassification would mainly depend on two variables, namely prevalence of adenomatous histotype and type of guidelines adopted. Similarly to advanced neoplasia prevalence, relative prevalence of adenomatous histotype within colorectal lesions is intimately related with polyp size, being about 50% and about 65% in diminutive and small lesions, respectively.7,59,60 Based on these values, when assuming a 90% EC-based sensitivity for adenomatous histotype, the negative predictive value for adenomatous histology would equalize a 90% threshold for diminutive lesions, but it would be substantially inferior for 6 to 9 mm polyps. When limiting our analysis to diminutive lesions, polyp prevalence is also likely to be related with polyp location. Because of the well-known prevalence of several tiny hyperplastic lesions in the rectosigmoid tract, the relative prevalence of adenomatous histotype may be expected to be further reduced in this tract, as compared with the remaining colon. In a consecutive series of 235 distal polyps - including 220 ≤5 mm lesions - only 38 were actually adenomatous, corresponding to a 16% overall frequency of the adenomatous histotype.9 Because of the inverse relationship between adenomatous prevalence and negative predictive value, the very low disease prevalence in the rectosigmoid tract further reassure on the safety of EC-based policies in this location. The clinical impact of eventual false-positive/negative results at EC would also depend on the type of guidelines adopted. According to the United States and European-based guidelines, patients with one to two tubular subcentimetric adenomas should have their next surveillance examination at 5 to 10 years and 10 years, respectively.5 The impact of this 5 to 10 year difference on the implementation of EC-based policies is dramatic. If a 5-year interval is chosen, any false-positive/negative result at EC would cause an inappropriate anticipated/delayed surveillance interval for hyperplastic and adenomatous lesions, respectively, underlining the necessity for an optimal EC-accuracy in this scenario. On the other hand, if a 10 year interval for patients with one to two tubular subcentimetric adenomas is adopted, any false-positive/negative result would not affect the 10-year surveillance interval, since adenomatous and hyperplastic lesions would share a common 10-year interval recommendation in this scenario. The final criticism to EC-based policies is represented by the impossibility of differentiating between hyperplastic and nonhyperplastic serrated lesions - such as sessile serrated polyps or sessile serrated adenomas lesions - at EC, because of the similar EC characteristics of these lesions.14 However, prevalence of sessile or traditional serrated adenoma has been shown to be very low in subcentimetric lesions, being cumulatively present in 0.3% to 0.5% and 0.8% to 1.3% of diminutive and small lesions, respectively.7,60 Moreover, these lesions seem to be associated with a higher risk of synchronous or metachronous advanced neoplasia only when located in the proximal colon or larger than 10 mm.61
Based on all these considerations, the American Society for Gastrointestinal Endoscopy (ASGE) recently developed a preservation and incorporation of valuable endoscopic innovations (PIVI) statement for real-time endoscopic assessment of the histology of diminutive colorectal polyps.62 In detail, it was determined that:
1) 'For colorectal polyps <5 mm in size to be resected and discarded without pathologic assessment, endoscopic technology (when used with high confidence) used to determine histology of polyps <5 mm in size, when combined with histopathologic assessment of polyps >5 mm in size, should provide a >90% agreement in assignment of postpolypectomy surveillance intervals when compared with decisions based on pathology assessment of all identified polyps.'
2) 'For a technology to be used to guide the decision to leave suspected rectosigmoid hyperplastic polyps <5 mm in size in place (without resection), the technology should provide >90% negative predictive value (when used with high confidence) for adenomatous histology.'
The ASGE, therefore, recommended two different EC-based policies, namely a predict-resect-and-discard strategy for nonrectosigmoid <5 mm lesions characterized at EC with high-confidence, and a predict-and-do-not-resect policy for rectosigmoid diminutive polyps predicted as hyperplastic at EC with high confidence. The overall algorithm is summarized in Fig. 1.62
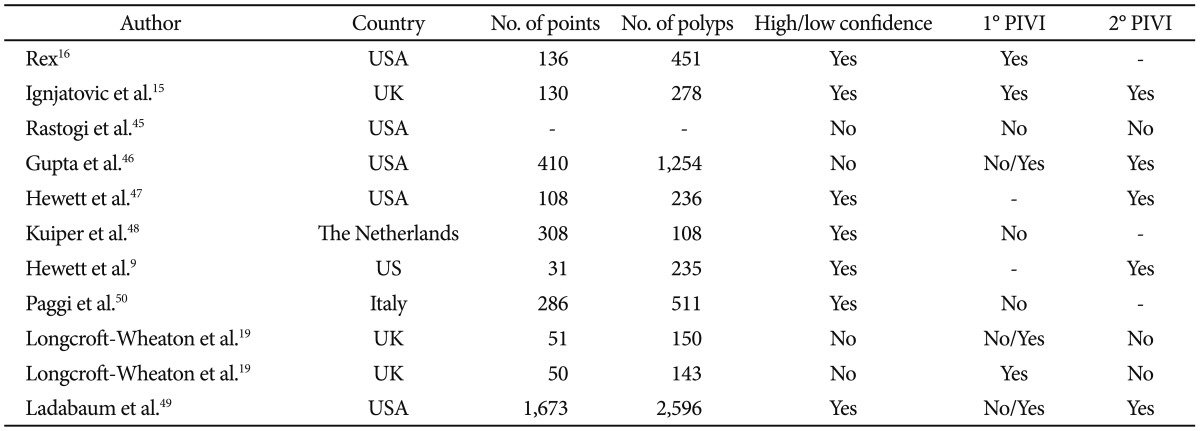
The ability of EC to meet with the 1° PIVI has been tested in a few series (Table 2).9,15,16,19,25,46-50 When recommending a 5-year interval surveillance for low risk subcentimetric adenomas,5 the majority of the available series failed to match the 1° PIVI, especially when EC was performed by less experienced endoscopists. On the other hand, when adopting a 10-year schedule, most of the studies succeeded in meeting the 1° PIVI. Intriguingly, when considering a 10 year interval for low-risk subcentimetric adenomas, a different strategy, in theory, would be to do-not-predict-resect-and-discard one to two diminutive lesions without EC-based prediction, reserving EC differentiation only to patients with at least three lesions. However, it is unclear whether the medical community would be ready to resect and discard lesions without having received any prediction about its histology.11
The 2° PIVI is rather innovative, since it introduces the predict-and-do-not-resect strategy based on the main assumption that - after EC-prediction of hyperplastic histotype - the possibility of leaving in situ a ≤5 mm adenoma is too low to warrant the cost of polypectomy itself. Therefore, the predict-and-do-not-resect policy represents a dramatic step forward in rationalizing the exploitation of medical and economic resources at colonoscopy, since it does not only exclude the pathological examination, but also the polypectomy itself from the colonoscopy procedure. When considering the low prevalence of adenomatous component among subcentimetric rectosigmoid lesions, it was not unexpected that the majority of the available studies consistently validated the feasibility of this policy, resulting into >90% negative predictive values. The exclusion from this strategy of nonrectosigmoid lesions may be also expected to marginalize the risk of leaving high-risk serrated lesions in situ. However, it could also be argued that the drawback of this policy is to accept that 1 in every 10 patients with a rectosigmoid polyp discarded at EC would remain in situ, resulting into the risk of progression of one unresected diminutive EC-misclassified adenoma. At this regard, previous studies addressed the natural history of unresected diminutive or larger lesions in the recto-sigmoid tract, reassuring on the very low risk of progression of these lesions. In detail, Hoff et al.63 and Hofstad et al.64 followed up 194 diminutive and 253 ≤10 mm polyps detected for 3 and 2 years, respectively. No diminutive polyp reached a >5 mm size and only 0.5% of ≤10 mm polyps eclipsed the 10-mm threshold after a 1-year time interval, and no case of severe dysplasia or carcinoma was registered.63,64 In a recent Japanese study only 2.9% of 408 subcentimetric lesions followed up for 43.1 months reached a ≥10 mm size, without the occurrence of any invasive cancer.65 Overall these data may be reassuring, when considering the very low risk of discarding an (advanced) adenoma in the rectosigmoid colon.
CONCLUSIONS
The increasing volume of colonoscopy procedures - related with a growing awareness of the efficacy of CRC screening - in a period of economic constraint requires a rational exploitation of the limited medical and financial resources. This is further worsened by the additional volume of surveillance procedure generated by the detection of neoplastic lesions at the screening examination, especially when considering the increase in adenoma detection rate with the evolution of endoscopic technology and the development of quality assurance programs. For this reason, any policy that may simplify and rationalize colonoscopy procedure or work up is useful. Predict-resect-and-discard and predict-and-do-not-resect policies offer the advantage of saving the cost for polypectomy or postpolypectomy pathological examination in a substantial percentage of the cases, as well as to recommend on the same day of the colonoscopy procedure the recommended surveillance interval. In order to meet the desired clinical thresholds, however, EC-based policies require a careful reassessment of the current postpolypectomy surveillance guidelines. When considering the intrinsic limit of EC-accuracy, the recommendation of a 10-year interval for low-risk adenomas would minimize any risk of EC-based false-positive/negative result, prompting for an immediate implementation of these new policies in clinical practice.

 XML Download
XML Download