

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Dental societies in the U.S. and Europe stress the importance of using a panoramic radiograph for surveying patients,1,2 and quality assurance guidelines for panoramic radiography are continuously being published and revised.3,4
In 2001 in South Korea, a special law to establish a legal basis for medical imaging quality control was enacted. Based on the law, regulation on the installation and operation of special medical instruments including computed tomography, magnetic resonance imaging, and mammography was enacted and published, which provided the legal groundwork for medical imaging quality control.5 However, continuous quality control of panoramic radiography, a frequently performed exam in dentistry, is in its beginning stage. In 2009, the Korea Food and Drug Administration initiated a study on the recommended radiation dose in panoramic radiography, and it is considered the first step in dental imaging quality control.6
Quality assurance of dental radiography consists of the inspection of the personnel and facility, as well as image quality assurance. The image quality assurance inspection consists of a clinical imaging evaluation and a standard phantom image test.7 Among the various types of image quality evaluation, clinical imaging evaluation is the most important inspection that enables actual and comprehensive evaluation since it reflects the entire quality assurance process, and it must be performed continuously.8
The panoramic radiographic unit uses both the principle of tomography and the principle of scanning. Characteristically, it may produce images that lack diagnostic value if the mandible and maxilla of interest are not correctly positioned in the focal trough.9
Recently, with the development of the image transmission system and the wide use of digital panoramic radiographic equipment, the quality of panoramic radiographic equipment has improved10 and consequently, a quality image can be obtained.
As no appropriate guidelines on quality control have been prepared in South Korea, related studies are required. A certified inspection method is required to appropriately and effectively maintain and control the image quality, and studies on the current status of the panoramic radiography of local dental hospitals and clinics are prerequisites for such a certified inspection method.7
The purpose of this study was to investigate the level of clinical image quality for panoramic radiograph and to provide a basis for clinical image evaluation, which is the most important part of quality assurance in South Korea.
Materials and Methods
Collection of images
Among the approximately 13,000 dental hospitals and clinics in South Korea, 260 (about 2%) were selected using the random sampling method, with the help of the Korean Dental Association. The 260 dental hospitals and clinics were asked to cooperate in the clinical image evaluation of panoramic radiographs.
Each dental hospital or clinic was asked to provide three randomly selected radiographs. The image identification such as the name and sex did not accompany the radiograph to protect the patient's privacy. The file format of the radiographs was limited to JPG or DICOM and they were sent by email as an attachment.
Training of clinical image evaluators
To ensure a professional and efficient evaluation, oral and maxillofacial radiology specialists or clinicians who had been working in a hospital's Department of Oral and Maxillofacial Radiology for five years or more evaluated the clinical images. During meetings for the pilot study, 14 evaluators were trained to evaluate panoramic images, and an agreement on the objective criteria for the qualitative evaluation of the images was forged among the evaluators.11
Clinical image evaluation using a clinical image quality evaluation chart
A chart was used to evaluate the image quality of a panoramic radiograph (Table 1). It was prepared during multiple meetings of evaluators. The perfect score in the clinical image evaluation was 100 points: 8 points for patient identification, 6 for artificial shadow, 8 for image coverage, 30 for patient positioning, 38 for image density, resolution, and contrast, and 10 for image quality grade.
One of the 14 evaluators evaluated an image using the aforementioned chart and calculated the total score. Since all of the information on the patients, hospitals or clinics, and equipment were excluded during the data collection process, all of the images got a full mark for the parameter of patient identification.
Classification of the overall image quality grade
Three clinical image evaluators classified the overall image quality of the panoramic radiographs. The evaluators evaluated the image quality while viewing the images; and if there was any inconsistency between their evaluations, an agreement was made through discussion. The image quality grade was classified into the following 4 grades: 1. optimal for obtaining diagnostic information, 2. adequate for diagnosis, 3. poor but diagnosable/unrecognizable, and 4. too poor for diagnosis. The detailed criteria are shown in Table 2.
For each image quality grade, the score was calculated according to the Clinical Image Quality Evaluation Chart, and scores of images that could be diagnosed were calculated according to the image quality evaluation chart by comparing the maximum and minimum scores.
Causes of imaging errors
Apart from the scores calculated by the three clinical image evaluators based on the image quality grade, the cause of the error observed on the image was determined and marked. The errors were classified into positioning errors during radiography (patient preparation, position of the mandible and maxilla, patient movement, and angle of the cervical spine), errors from the radiographic unit and other mechanical errors (irregularity of the exposure roller and error of the sensor and reader), pre- and post-processing errors (enhancement errors, noise, and abnormal density and contrast), and errors due to anatomic abnormality (malformation of the mandible and maxilla, and congenital dental anomaly).
Results
Image collection
The images were collected from a total of 99 dental hospitals and clinics. The response rate was 38.1% and a total of 297 panoramic radiographs were collected, from which nine were excluded due to transmission error and 288 were included.
Clinical image evaluation and classification of overall image quality grade
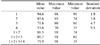
The mean of the scores given by a single specialist according to the Clinical Image Quality Evaluation Chart was 79.9 (maximum possible: 100), with the highest and lowest scores 98 and 35, respectively. The mean and representative scores of each group based on the overall image quality grade, the last parameter, are shown in Table 3.
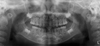
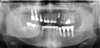
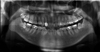
In the classification of the overall image quality by the three evaluators, 17 images were deemed 'optimal for obtaining diagnostic information,' 153 were 'adequate for diagnosis,' 109 were 'poor but diagnosable,' and nine were 'unrecognizable and too poor for diagnosis' (Figs. 1, 2, 3, 4).
About 59.0% (170) of all the images were rated 'optimal for obtaining diagnostic information' or 'adequate for diagnosis' (Table 4). About 96.9% (279) of the images had a 'poor but diagnosable' or better image quality.
The mean scores of the images with the image quality of 'optimal for obtaining diagnostic information' and 'adequate for diagnosis' were 15 points higher than that of the images with 'poor but diagnosable' image quality, and the lowest score (74 points) of the images with the 'adequate for diagnosis' image quality was higher than the mean scores of the images with a 'poor but diagnosable' image quality.
Some images scored higher than the mean score of the images with an 'adequate for diagnosis' image quality but were graded with a 'poor but diagnosable' image quality because of the difference in their left and right contrasts due to inappropriate posture, a too dark or too white image, and an intensive burnt-out spot in the area of the inferior border of the mandible or soft tissue due to the intense contrast, though the image could be interpreted (Fig. 5).
In particular, the panoramic images that scored 80 points, the highest for the images with a 'poor but diagnosable' image quality, were graded to have a poorer than 'adequate for diagnosis' image quality despite their higher score since it was impossible to evaluate the condylar area and the inferior area of the mandible because the top and bottom and the left and right of the image coverage were all not imaged, despite the good image quality of the teeth area (Fig. 6).
Causes of the clinical image errors
The results of the analysis of the causes of the errors in all the images are as follows (Table 5). There were 139 errors in the positioning, such as the patient positioning, patient movement, and angle of the cervical spine; 135 errors in the processing such as an abnormal density, contrast, and resolution; 50 errors from the radiographic unit and other mechanical problems; and 13 errors due to anatomic abnormality. The total number of errors is not the same as the total number of images because some images had multiple errors and some had no errors at all.
The most common errors in the images with an 'adequate for diagnosis' image quality were errors in positioning and errors of image taking, followed by processing errors, mechanical errors of the radiographic unit, and errors due to anatomic abnormality. In contrast, images with a 'poor but diagnosable' image quality had more preprocessing errors than positioning errors.
Nine images with an 'unrecognizable, too poor for diagnosis' image quality had image errors due to the causes shown in Table 5; i.e., four images had positioning errors alone in the image taking, five images had both mechanical errors of the radiographic equipment and processing errors, and no image had errors due to anatomic abnormality.
The errors in image taking mostly involved considerable deviation of the patient posture from the normal patient posture. The mechanical and processing errors were caused by the irregularity in the image due to the irregular roller speed, abnormal exposure, and density abnormality (such as a too dark or too light image) that occurred all together.
Discussion
This study investigated the image quality of panoramic radiographs taken at dental hospitals and clinics across Korea. Clinical images were evaluated and scored using a Clinical Image Quality Evaluation Chart. The mean score of the images was 79.9 out of the highest possible score of 100. Considering that 75% of the reference dose was used, the score would be 88, and thus, 88 points can be recommended.
In addition to the evaluation using the Clinical Image Quality Evaluation Chart, the images were also classified into four grades, and 59.0% of the images had a normal or higher-level image quality. Considering that the mean score of the panoramic radiographs taken at local dental hospitals and clinics based on the image quality evaluation was 79.9 points, which is higher than the lowest score (74 points) of the images with a normal image quality, and that more than half of the images had a normal or higher-level image quality, the image quality of the panoramic radiographs taken at local dental hospitals and clinics had a normal or higher-level image quality.
On the Clinical Image Quality Evaluation Chart, the necessary parameters to be fulfilled should be pointed out clearly in order to prevent 'unrecognizable, or too poor for diagnosis' images from achieving scores above the reference level. The parameters that need to be met must be selected, and the images should be graded as 'unrecognizable and too poor for diagnosis' when the necessary parameters are not met regardless of the results for the other parameters. In this study, we tried to solve this problem by including the overall image quality grade in the Clinical Image Quality Evaluation Chart.
The images with an overall image quality grade that was lower than the scores based on the Clinical Image Quality Evaluation Chart had errors due to the following: as described in the Results section, the top and bottom and the left and right sides cut from the area of the image; the interpretation of the anterior teeth area was impossible due to malpositioning; and there was severe contrast abnormality due to a too dark or too white image. These factors have greater influence on the image quality than other factors and can thus be considered parameters that need to be met.
Also, in many cases, the cause of the error was not consistent among the three images sent from each hospital or clinic. The causes were as follows: (1) the patient age and body condition were different; (2) the patient positioning was not uniform during the image taking; and (3) even if the patient positioning was appropriate, the conditions of the radiographic unit could have been different if the images were taken on different days.
The cause of the error differed by grade. For the images with an 'adequate for diagnosis' image quality, positioning errors in the image taking were most common, followed by preprocessing errors, radiographic camera errors, and errors due to anatomic abnormality. In contrast, for the images with a 'poor but diagnosable' image quality, preprocessing errors were more common than positioning errors. This could have been due to the following: during the image taking, such devices as the bite block, chin rest, and head rest were used to fix the patient's head so as to minimize the possibility of a positioning error, whereas the processing error is attributable to mechanical and software problems and thus, the range of problems is unlimited.
This indicates that processing problems have a worse effect on the interpretation of the image than positioning errors. As such, the results of the analysis of the errors indicated that management and training of relevant personnel and inspection of facilities are required.
This study is meaningful because it is the first study that investigated the current status of panoramic radiographs taken at local dental hospitals and clinics and that evaluated the quality of clinical images to promote quality assurance in panoramic radiography.
In conclusion, panoramic radiographs taken at local dental hospitals and clinics generally have a normal or higher-level image quality. Principal factors affecting image quality were, namely, positioning of the patient and image density, sharpness, and contrast. Therefore, when images are taken, patient position should be adjusted with great care. Also, standardizing objective criteria of image density, sharpness, and contrast would be required to evaluate image quality effectively. Images with a below-normal image quality are not adequately addressed, however, because of lack of regulations on equipment and image quality assurance in panoramic radiography. Currently, in the beginning stage of panoramic radiography, quality assurance systems for dental radiography are being prepared, and specialists of the Korean Academy of Oral and Maxillofacial Radiology, the main body for dental radiography, are actively participating in quality assurance development and implementation. Guidelines are needed on image quality management for panoramic radiography to promote public health and reduce medical costs.







 XML Download
XML Download