

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
For successful endodontic treatment, the root canal system should be isolated from the periodontal ligament space and bone by sealing it completely with an appropriate root filling material. Thereby, endodontic effects that threaten the health of periapical tissues can be eliminated.1 The main aim of root canal treatment is completely removing debris and microorganisms from root canal system and then filling it with a material which is biologically inert and has stability in length.2
Successful endodontic treatment mainly depends on disinfection of the root canal system, prevention of leakage of bacteria from the oral environment to the periapical tissues, and the complete filling of the root canal system until the apical constriction in three dimensions with an inert, stable in length, and biologically coherent material.3 Properly performed root canal fillings also prevent contamination with bacteria from coronal leakage.4 Ideal root canal filling material should adapt to the root canal wall perfectly and all canals should be filled with homogenized gutta-percha.5
Two-dimensional conventional and digital intraoral radiography are most commonly used for the assessment of endodontic treatments. Digital radiography was shown to be beneficial in endodontic treatments. Regardless of the intraoral system used, the two-dimensional nature of images limits the information that can be obtained and their diagnostic value is dependent upon beam angulation, superimposition of anatomical structures, and patient-related factors.6 Upon radiographic evaluation, depending on the X-ray beam angulation and tooth position, even an improper root canal treatment with insufficient condensation and adaptation can be assumed appropriate.7 Conventional intraoral film consists of silver halide crystals in order to produce analog images. On the other hand, digital intraoral systems include a photostimulable phosphor-coated plate (PSP), a solid state silicon chip such as a charge-coupled device (CCD), and a complementary metal oxide semiconductor (CMOS) that uses a scintillator layer to convert X-rays to light. PSP absorbs and stores the energy from X-rays. This energy is released as phosphorescence when stimulated by another light of an appropriate wavelength. These systems offer reduced radiation dosage, shorter exposure time, image enhancement, and ease of storage, retrieval, and communication.8-10
Recently, portable hand-held dental X-ray units have become available in the dental field. Their small camera-like design and light weight make them easy to use, especially for forensic and military purposes. Their integrated battery supplies the electrical power for convenient cordless operation. Furthermore, this wireless power supply makes the devices more independent of fixed electric current sources. Together with digital image sensors, this type of machine ensures quick and fully digitized data collection.11,12 A previous study found that the use of a NOMAD hand-held device resulted in a very low radiation exposure to the patient and operator, and the measured doses were below recommended limits.13
There are also numerous film-based and digital panoramic systems in routine clinical practice. Panoramic radiography is a simple method of obtaining images by synchronous rotation of the X-ray source and image receptor around the stationary patient. Broad coverage of both jaws and teeth are obtained without anatomical detail available on intraoral periapical radiographs.14-16
If two-dimensional conventional radiographic methods are insufficient and fail to provide the necessary information, cone beam computed tomography (CBCT) imaging should be taken into consideration.17 CBCT uses a cone-shaped X-ray beam centered on a two-dimensional (2D) sensor to scan a 180°-360° rotation around the patient's head to acquire a full 3D volume of data. The main advantage of using CBCT for endodontic applications is that it can provide three dimensional (3D) views which intraoral and panoramic radiography cannot provide.17,18 Although CBCT eliminates many disadvantages of intraoral radiography, it must be taken into consideration that the patient receives higher radiation doses compared with intraoral and panoramic radiography. Therefore, the CBCT should be used only if conventional methods are not useful for diagnostic accuracy.17,18
Considering the importance of radiographic root canal treatment assessment and possible differences between various radiographic methods, the aim of this ex vivo study was to assess the diagnostic potential of intraoral conventional and digital radiography, panoramic radiography, and CBCT in the detection of teeth with ideal or non-ideal root canal treatment.
Materials and Methods
Our study included 120 mandibular incisors (n=48), canines (24), and premolars (48), single rooted teeth with and without dental caries that had been extracted for periodontal or orthodontic reasons. The teeth were cleansed of calculus and debris, disinfected in 2% NaOCl solution for 20 minutes and stored in distilled water. Root pulps were removed by use of trinerve. Afterwards, the working length was determined with a #15 H file and was pushed to the foramen until the file was visible and then pulled back 1 mm. A #40 H file at the apical third and a #80 H file at the coronal third were used with the step back technique. During the preparation, the root canals were irrigated with 2 mL EDTA and 2 mL 2.5% NaOCl using dental injectors. Finally, 2 mL 2.5% NaOCl, 2 mL saline, 2 mL 17% EDTA, and 2 mL saline were applied. After irrigation, all of the canals were dried with paper points (Sure-endo, Sure Dent Corp., Seongnam, Korea).
The teeth were divided into four groups according to the type of root canal treatment applied: (1) ideal root canal treatment (60 teeth), (2) insufficient lateral condensation (20 teeth), (3) root canals filled short of the apex (20 teeth), and (4) overfilled root canals (20 teeth). All of the specimens were filled with AH26 (Dentsply Maillefer, Tulsa, OK, USA) and gutta percha with the lateral condensation technique according to its group specifications. After the gutta percha was cut, all of the specimens were stored in petri plates with damp cotton at 37℃ to harden the root canal filling material. Randomly selected teeth were placed in the appropriate sockets of dry mandibles in groups of 10 (four incisors, two canines, and four premolars) with their crowns visible and proximal surfaces in contact where possible. The selected dry mandible had two molars on the right and one molar on the left side. A 2 cm thick plastic glove filled with distilled water was placed around the dry mandible in order to simulate soft tissue. The teeth were imaged by use of the following methods: 1. intraoral conventional radiograph using film, 2. panoramic radiograph using film, 3. digital intraoral systems (CCD and PSP), 4. direct digital radiograph (CCD) obtained with portable X-ray unit, 5. digital panoramic radiograph, and 6. CBCT images obtained with 0.3mm3 and 0.2mm3 voxel size. All intraoral images were obtained with a standardized paralleling technique and a focus-receptor distance of 30 cm.
1. Intraoral conventional radiographs were taken using a Heliodent DS (Sirona, Bensheim, Germany) X-ray unit operated at 70 kVp and 7 mA for 0.40 seconds with Kodak (Kodak, Rochester, NY, USA) E-speed (#2 sized) film.
2. Conventional panoramic radiographs were taken using a Planmeca Proline (Planmeca Co., Helsinki, Finland) operated at 75 kVp and 10 mA.
Intraoral and panoramic films were processed immediately after exposure using a Velopex, (Extra-X Medivance Instruments Ltd., London, UK) automatic processing machine and fresh chemicals according to the manufacturer's specifications.
3. Digital intraoral images were obtained with the same X-ray unit used for film images, Heliodent DS (Sirona, Bensheim, Germany) operated at 70 kVp and 7 mA. The digital intraoral systems were a Dr. Suni (#1 sized) direct digital intraoral CCD sensor (Suni Medical Imaging, San Joe, CA, USA) with 0.08 seconds exposure time and a #2 sized Digora Optime (Digora, Tuusula, Finland) PSP digital intraoral system, which included a feature that automatically erased residual image signals with 0.08 seconds exposure time. The exposed phosphor plates were scanned immediately after exposure.
4. Direct digital radiograph (DDR) obtained with portable X-ray source technique
Direct digital intraoral images were also obtained using a #1 sized Dr. Suni direct digital intraoral CCD sensor with a portable X-ray unit Dexcowin DX3000 (Dexcowin Co., Seoul, Korea) operated at 60 kVp and 1 mA for 0.08 seconds.
5. Digital panoramic radiography
Digital panoramic images were exposed with a Planmeca Proline XC (Planmeca Co., Helsinki, Finland) panoramic X-ray unit operated at 60 kVp and 4 mA.
6. CBCT images
CBCT images were obtained using an ILUMA ultra cone beam CT scanner (3M Imtec, Ardmore, OK, USA) with a 24.4×19.5 cm amorphous silicon flat-panel image detector and a cylindrical volume of reconstruction up to 21.2×14.2 cm. Images were obtained at 120 kVp, 3.8 mA with an exposure time of 40 seconds. Thereafter, volumetric data were reconstructed with voxel sizes of 0.3 mm3 and 0.2 mm3 to provide serial coronal and sagittal sections.
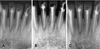
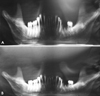
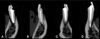
Figure 1 shows the examples of the intraoral radiographs of the mandibular teeth with different root canal treatments applied. Figures 2A and B show the conventional and digital panoramic images, respectively, of the same group of teeth shown in Figure 1. Figure 3 shows the images obtained with a CBCT unit reconstructed by 0.2 mm3 voxel of the teeth shown in Figure 1.
All images were evaluated separately by two oral radiologists and one endodontist. The intra-observer agreement was assessed by having each observer view all of the images twice, with a two week interval between viewings to eliminate memory bias. All of the observers were informed of the evaluation criteria. All of the images were viewed at random in a dimly lit room. The visibility of the enamel, bone trabeculation, and dentine were used as the indicators of image quality for all imaging techniques and were decided upon with the consensus of all of the observers. The conventional images were evaluated against a light box using a 2× magnifier. All digital images were evaluated on a 17 inch Philips Energy Star monitor (Philips Electronics Industries Ltd., Taoyuan County, Taiwan) set at a screen solution of 1,440×900 pixels and 32 bit color depth using each system's own software and enhancement tools.
The weighted kappa coefficients were calculated to assess intra- and inter-observer agreements for each image set. Kappa values were calculated according to the following criteria: <0.10, no agreement; 0.10-0.40, poor agreement; 0.41-0.60, significant agreement; 0.61-0.80, strong agreement; 0.81-1.00, excellent agreement, and these values were calculated by MedCalc statistical software (MedCalc Software, Mariakerke, Belgium). For all observer assessments, the percentage of correct readings obtained from each modality was calculated for each root canal treatment type. SPSS 15.0 (SPSS Inc., Chicago, IL, USA) was used for analyses and the t-test was used for comparison of modalities with the significance level set at p<0.05.
Results
The intra-observer kappa coefficients calculated for each observer using the radiological method ranged between 0.327 and 0.849, showing, in general, strong agreement (Table 1). The inter-observer kappa coefficients calculated for each observer using the radiological method for the first readings ranged between 0.312 and 0.748, showing significant agreement (Table 2). The inter-observer kappa coefficients calculated for each observer using the radiological method for the second reading ranged between 0.369 and 0.749; again strong inter-observer agreements were found for all methods showing significant agreement (Table 3). The significant Kappa values obtained from the observers' correct assessment percentage obtained for each root canal treatment type by imaging modality were taken into consideration for all observers.
Table 4 shows the correct assessment percentage for the teeth with ideal root canal treatment. For the teeth in the ideal root canal treatment group, the CBCT with 0.2mm3 voxel images revealed the best results, while the portable X-ray with CCD had the worst results: CBCT (0.2 mm3)>digital panoramic>conventional panoramic>PSP>conventional periapical film>CBCT (0.3 mm3)>CCD>portable X-ray with CCD. Statistically significant differences were found between CBCT (0.3 mm3) and both the portable X-ray with CCD (p=0.01) and CBCT (0.2 mm3) (p=0.004). There were statistically significant differences between digital panoramic and both CCD with a fixed X-ray source (p<0.001) and portable X-ray with CCD (p<0.001). There were also significant differences between CBCT (0.2 mm3) and all of the following: PSP (p=0.03), CCD (p<0.0001), portable X-ray with CCD (p<0.0001), and conventional periapical film (p=0.009). Statistically significant differences were found between conventional periapical film and both CCD with a fixed X-ray source (p=0.047) and portable X-ray with CCD (p=0.009). There were also significant differences between conventional panoramic and both CCD with a fixed X-ray source (p=0.003) and portable X-ray with CCD (p<0.001). In addition, significant differences between PSP and both CCD with a fixed X-ray source (p=0.01) and portable X-ray with CCD (p=0.002) were found.
Table 4 shows the correct assessment percentage for teeth with insufficient lateral condensation. The assessment of teeth with insufficient lateral condensation showed the most correct percentage of readings for conventional periapical film followed by CCD and PSP. The lowest percentage of correct assessments was obtained with digital panoramic followed by CBCT at 0.3mm3 voxel resolution and conventional panoramic: film>PSP=CCD>portable X-ray with CCD>CBCT (0.2mm3)>conventional panoramic> CBCT (0.3 mm3)>digital panoramic. Statistically significant differences were found between the conventional periapical film and both CBCT at 0.2mm3 (p=0.0076) and CBCT at 0.3mm3 (p<0.001). Statistically significant differences were also found between digital panoramic and all of the following: portable X-ray with CCD (p=0.032), digital panoramic and CCD with a fixed X-ray source (p=0.004), digital panoramic and PSP (p=0.004), and digital panoramic and conventional periapical (p<0.001). There were statistically significant differences between conventional panoramic and the following: CCD (p=0.02), PSP (p=0.02), and conventional periapical film (p=0.002). In addition, significant differences between CBCT at 0.3mm3 and both CCD (p=0.006) and PSP (p=0.006) were found.
Table 4 shows the correct assessment percentage for teeth with root canals filled short of the apex. Assessment of teeth with root canals filled short of the apex showed the highest percentage of correct readings for CBCT images and CCD images. The lowest percentage of correct assessments was obtained with the conventional and digital panoramic images: CBCT (0.2mm3)=CBCT (0.3mm3)=CCD>PSP=film>portable X-ray with CCD>digital panoramic>conventional panoramic. Statistically significant differences were found between conventional panoramic film and all of the following: CBCT at 0.2mm3 (p=0.005), CBCT at 0.3 mm3 (p=0.005), portable X-ray with CCD (p=0.048), CCD with a fixed X-ray source (p=0.005), PSP (p=0.02), and conventional periapical film (p=0.02). Statistically significant differences were also found between the digital panoramic and both CBCT at 0.2mm3 (p=0.01) and CBCT at 0.3mm3 (p=0.01).
Table 4 also shows the correct assessment percentage for teeth with overfilled root canals. For the overfilled root canal treatment group, PSP images and conventional periapical film radiographs had the best scores whereas CBCT at 0.3 mm3 and digital panoramic images had the lowest scores (PSP>Film>CCD>portable X-ray with CCD>conventional panoramic>CBCT(0.2mm3)>digital panoramic>CBCT (0.3 mm3)). Statistically significant differences were found between CBCT (0.3 mm3) and the following: portable X-ray with CCD (p=0.002), CBCT (0.3 mm3) and CCD with a fixed X-ray source (p<0.001), CBCT(0.3mm3) and PSP (p<0.001), and CBCT (0.3mm3) and conventional periapical film (p<0.001). There were also statistically significant differences between the digital panoramic and the following: conventional periapical film (p=0.01), PSP (p=0.007), and CCD with a fixed X-ray source (p=0.02). In addition, significant differences between CBCT at 0.2mm3 and both CCD (p=0.006) and PSP (p=0.03) were found.
Discussion
The aim of the present study was to assess the accuracy of root canal treatment with several radiographic techniques used in clinical dentistry. The present research found different results for different methods for different canal treatment options. To our knowledge, this study was the first trial to compare CBCT with different two-dimensional techniques in terms of root canal filling accuracy. Although we found a higher percentage of correct readings for CBCT compared to other modalities when evaluating teeth with root canals filled short of the apex, CBCT was inferior to intraoral modalities when evaluating teeth with overfilled root canal fillings and teeth filled with insufficient condensation.
A significant issue that can affect the image quality and diagnostic accuracy of CBCT images is the scatter and beam hardening artifacts caused by high density adjacent structures, such as metal posts, restorations, and root filling materials.19 However, it is clear that there are many specific situations where the 3D images produced by CBCT facilitates diagnosis and influences treatment. The usefulness of CBCT cannot be disputed. It is a valuable task-specific imaging modality, producing minimal radiation exposure to the patient and providing maximal information to the clinician. Clinicians should use CBCT only when the need for imaging cannot be met adequately by lower dose conventional dental radiography or alternate imaging modalities.20
The image quality of panoramic radiographs taken digitally and conventionally was found to be similar.21 It has been suggested that panoramic radiographs cannot be used alone in order to detect perapical lesions, marginal bone loss, or caries.22 In our study, conventional panoramic radiographs were incompetent especially in the detection of insufficient lateral condensation and overfilled root canal treatment. Although panoramic radiography is not the method of choice for the assessment of root canal treatment, it is commonly available in routine practice and is especially useful when a broad view of both jaws is required. It was very difficult to standardize images by placing the mandible in the focal trough, as mentioned above, especially in this ex vivo model. However, we assessed the panoramic images because of their frequent use in clinical practice. The high percentage of correct assessments for ideal root canal treatment may be due to the fact that with panoramic imaging observers were unable to assess the anterior area and they readily rated most canals as ideally filled.
The image quality to detect the periodontal ligament, root ending, and bone trabeculations was better in conventional radiographs than conventional panoramic radiographs. However, in terms of the image quality of root canal morphology and endodontic filling materials, there were no differences between those methods.23 We found that there were no statistically significant differences between conventional periapical radiographs and conventional panoramic radiographs for the assessment of ideal root canal treatment (p>0.05).
A study24 compared digital images obtained with a portable X-ray source (ADX-4000) and conventional bitewings according to their diagnostic quality. Digital 3.5 inch images were displayed on the built-in monitor of the ADX 4000 and digital 17 inch images were viewed on a 17 inch monitor; both methods had similar results.24 In a similar study, it was found that a combination of Nomad® with PSP gave the best scores for image MinRay®, AnyRay®, and Rextar® X-Ray devices in combination with PSP, CCD, or CMOS sensors.11 Another study revealed that images have better quality with a combination of a fixed X-ray source and PSP than with portable X-ray units.12 Also, it was found that radiological image quality was significantly higher for the phosphor quality, and Rextar® with Sopix2® was the best option to enhance portability.11 The authors also found that the combination of Nomad® with PSP showed the best results for image quality compared with the CMOS digital receptor system.12 In the present study, a portable X-ray unit was used with a CCD sensor. We obtained similar results with a portable X-ray unit and CCD compared with CCD with a fixed X-ray unit and PSP for root canal treatment assessment.
For the evaluation of root canal length with endodontic files, conventional radiographs showed better scores than PSP (Digora Optime-Digora, Tuusula, Finland) and RVG (Trophy, Vincennes, France) images.25,26 In the present study, in assessment of root canal treatment, there was no statistically significant difference between phosphor plate images and conventional radiographs (p>0.05).
A study revealed that PSP plates showed better image quality than CBCT. This might originate from the higher spatial resolution obtained with Digora Optime compared with CBCT.27 These results were in line with our findings, which suggested that phosphor plate images were better than CBCT images for the assessment of the insufficient lateral condensation and overfilled root canal treatment groups.
A previous study showed that for the detection of external root resorption, CBCT (0.3mm3 resolution) is the best option when exposure dosage is considered.28 We obtained CBCT images with 0.2 mm3 and 0.3 mm3 resolution. In the present study, CBCT images obtained with 0.2 mm3 voxels were, in general, better than the CBCT images obtained with 0.3mm3 voxels, which may be explained by better visibility of the root canals due to the smaller voxel size.
A study found that the ratio of the detection of root canal treatment 1-2 mm short of the apex using periapical radiographs was 88%, 89.3%, and 95% for the anterior, premolar, and molar, respectively, but the ratios for CBCT were 70%, 73.7%, and 79%.29 In our study, the assessment of teeth with root canals filled short of the apex showed the best correct percentage of readings for CBCT images at both voxels and for CCD images. The lowest percentages of correct assessments for short root canal fillings were obtained with conventional and digital panoramic images. Also, we obtained the best results for all systems when assessing teeth with root canals filled short of the apex. Since the canal treatment was shorter than 2 mm from the apex, it was easier to detect and observers mainly focused on the canal treatment shortage.
In a study aiming to evaluate the gaps in root canal treatment, it was found that gaps greater than 350 microns can be visualized by all imaging techniques, but for smaller gaps, the intraoral digital technique had better scores than the analog technique and CBCT imaging.30 In our study, the assessment of teeth with insufficient lateral condensation showed the highest percentage of correct readings using conventional periapical film, followed by CCD and PSP. The lowest percentage of correct assessments was obtained with digital panoramic radiography, followed by CBCT at 0.3mm3 voxel resolution and conventional panoramic radiography. However, we did not assess the dimensions of the gap with objective criteria; only observers' readings were assessed. Therefore, our results were more subjective.
A study compared root canal treatments according to their length and homogeneity. For single-rooted teeth, PSP image quality was found to be equal to conventional radiography and to be better than CBCT.31 In line with this study assessing insufficient lateral condensation, our study showed that PSP image quality was similar to CCD and better than CBCT images. The spatial resolution of Digora Optime (PSP) is 12.5 lp/mm and CBCT images are 2 lp/mm. This is likely to be the reason for the difference.
For tooth and root length measurement, CBCT produced more accurate results than periapical radiographs, and also 0.2, 0.3, and 0.4 mm3 resolution CBCT images were not statistically different.32 This study demonstrated that there was not a statistically significant difference between 0.2 mm3 and 0.3 mm3 resolution CBCT images only when assessing teeth in the root canal treatment short of the apex group. In the other assessment groups, 0.2mm3 voxel images outperformed 0.3mm3 voxel resolution images.
Although CBCT has the strong potential to replace intraoral techniques for the assessment of teeth in three dimensions, higher radiation doses, lower resolution and lack of availability compared to two-dimensional systems precludes its routine use. Newer CBCT systems offer the advantage of narrow field imaging with lower doses and better image quality.
In conclusion, the CBCT chosen for this study was found to be successful in the assessment of teeth with ideal root canal treatment and teeth with canals filled short of the apex. However, CBCT revealed inferior results compared to intraoral techniques when assessing teeth with insufficient condensation and teeth with overfilled canal treatment.




 XML Download
XML Download