

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Stroke is one of the most important issues encountered by the world's aging population and it is a leading cause of long-term disability [1]. Among many symptoms of stroke, motor recovery may be the most important aspect in stroke patients for performing functionally independent activities of daily life. Actually, it has been reported that motor impairment is one of the most serious disabling sequelae of stroke, with more than 50% of stroke patients experiencing a residual motor deficit [2]. To establish a proper rehabilitation plan for motor impairment, many studies were conducted to predict outcomes of motor function using various tools. Lesion localization and functional reorganization revealed possible predictive tools using various imaging studies [345]. Usefulness of diffusion tensor tractography to predict motor recovery has also been investigated in many studies [6]. Furthermore, transcranial magnetic stimulation (TMS)-induced motor evoked potentials (MEP) performed during hospital admission can be the method to predict functional recovery [78910]. In general, responsiveness of MEP is an important prognostic factor to predict motor recovery in stroke patients [7891011121314].
TMS-induced MEP can provide several quantitative parameters such as resting motor threshold (rMT), amplitude, volume of the MEP output curve, intracortical inhibition (ICI) and intracortical facilitation (ICF). Previous studies revealed that a high rMT could be associated with poor motor functional outcomes [15]. Several studies showed that the amplitude or amplitude ratio could be used for predicting motor functional outcomes [910]. The MEP amplitude has been used as a neurophysiological measure of corticomotor excitability [16]. The MEP output curve refers to the increase in MEP amplitude with increasing stimulus intensity of MEP. It can assess neurons that are intrinsically less excitable or spatially further from the center of activation by TMS [17]. As compared with many studies indicating a correlation between functional outcome and responsiveness or rMT of MEP, there have been few studies investigating other quantitative parameters of MEP as predictors of motor functional outcome and their results were incongruent. Therefore, the objective of this study was to reveal the usability of TMS-induced MEP in the early subacute phase to predict motor functional outcomes. For this purpose, we analyzed the relationships between the results of TMS-induced MEP in the early subacute phase and motor function at 3 months in stroke patients.
MATERIALS AND METHODS
Subjects
This study was a retrospective study performed using medical records of patients who suffered a stroke and were admitted to Samsung Medical Center. Inclusion criteria were patients who had (1) unilateral stroke lesions, (2) undergone motor functional evaluation at 3 months after stroke, (3) been transferred to the department of rehabilitation within 3 weeks after stroke onset, and (4) received TMS-induced MEP to evaluate cortical excitability within 3 weeks after stroke onset. In the present study, the 'early subacute phase' is defined as from 1 week to 3 weeks after stroke onset.
The exclusion criteria were patients who (1) suffered recurrent stroke, (2) were diagnosed with bilateral lesions by MRI or CT, (3) had other major neurological disease which could affect the patients' function. A total of 113 patients (61 men, 52 women; mean age 57.8±12.2 years) who suffered a first-ever stroke were included in the study.
TMS-induced MEP
For performing single-pulse TMS-induced MEP, the patients were seated in a reclining armchair with both hands pronated. Electromyography (EMG) data were recorded from the contralateral first dorsal interosseous muscle via surface electrodes. EMG activity was amplified using the Medelec Synergy EMG/EP system (Medelec, Oxford, UK), and the data were bandpass filtered at 10–2,000 kHz. Using a TMS system (Magstim BiStim2; Magstim Ltd., Carmarthenshire, UK) and a 70-mm figure-of-eight coil, the optimal scalp location was determined. The electromagnetic current would flow perpendicular to the central sulcus because the handle of the coil was oriented 45° posterior to the midline [1819]. Next, a single-pulse TMS was repeatedly applied to that location to determine each patient's rMT, defined as the lowest intensity of stimulus necessary to produce a MEP peak-to-peak amplitude ≥50 µV in five out of the 10 consecutive trials. The rMT provides information about a central core of neurons in the muscle representation in the motor cortex and it likely reflects neuronal membrane excitability [20]. To verify whether the patient was relaxed prior to stimulation, the examiner monitored muscle activity by real-time EMG. Absent MEP was defined when it failed to appear after 3 successive discharges with maximal output.
We also evaluated the amplitude of MEP at 100%, 110%, 120%, 130%, 140%, and 150% of the rMT, latency of MEP, volume of the MEP output curve, and recruitment ratios by applying various stimulation intensities, respectively. For each intensity of the rMT, five sweeps of the MEP were collected, and the mean amplitude of the MEP was calculated [21]. In all patients, each single-pulse TMS-induced MEP was performed in both the affected and unaffected hemispheres using the same protocol.
For paired-pulse TMS-induced MEP, MEP amplitude could be changed depending on the interval between conditioning stimulus and test stimulus. In the present study, paired stimulations were delivered at 2 ms and 4 ms intervals for triggering ICI and at 10 ms and 15 ms intervals for triggering intracortical facilitation (ICF), respectively. Intensities of conditioning and test stimulus were 80% and 120% of the rMT. Reductions or increases in the test stimulus by conditioning pulse were expressed as a percentage of the unconditioned MEP amplitude [22].
Motor function assessment
Primary outcome of this study was each patient's motor function, which was measured by Fugl-Meyer Assessment scale (FMA). The FMA used in our study consisted of an upper extremity score (FMA-UL), a lower extremity score (FMA-LL), and the total score (FMA-T; the sum of both the upper and lower extremity scores). We assessed each participant's motor function in the early subacute phase and at 3 months after stroke.
Statistical analysis
Data analysis was carried out using IBM SPSS ver. 22 software (IBM, Armonk, NY, USA). We classified stroke patients into the MEP response group and the MEP non-response group according to the presence of MEP in the affected hemisphere. In the MEP response group, we also calculated the ratio of parameters of TMS-induced MEP between both sides to evaluate the imbalance of cortical excitability. We defined the ratio of each parameter by calculating the difference between both sides (value of the affected side/value of the unaffected side). The Shapiro-Wilk test was used to determine the distributional normality of all continuous variables (all variables were found to be normally distributed; p<0.05). Independent t-tests and chi-square tests were used to compare the parameters between the MEP response and MEP non-response groups. In the MEP response group, correlation analysis was used to assess the correlation between motor function and MEP parameters. After correlation analysis, multiple regression analysis with significant variables was used to identify the meaningful independent prognostic factor. The p-values less than 0.05 were considered statistically significant.
RESULTS
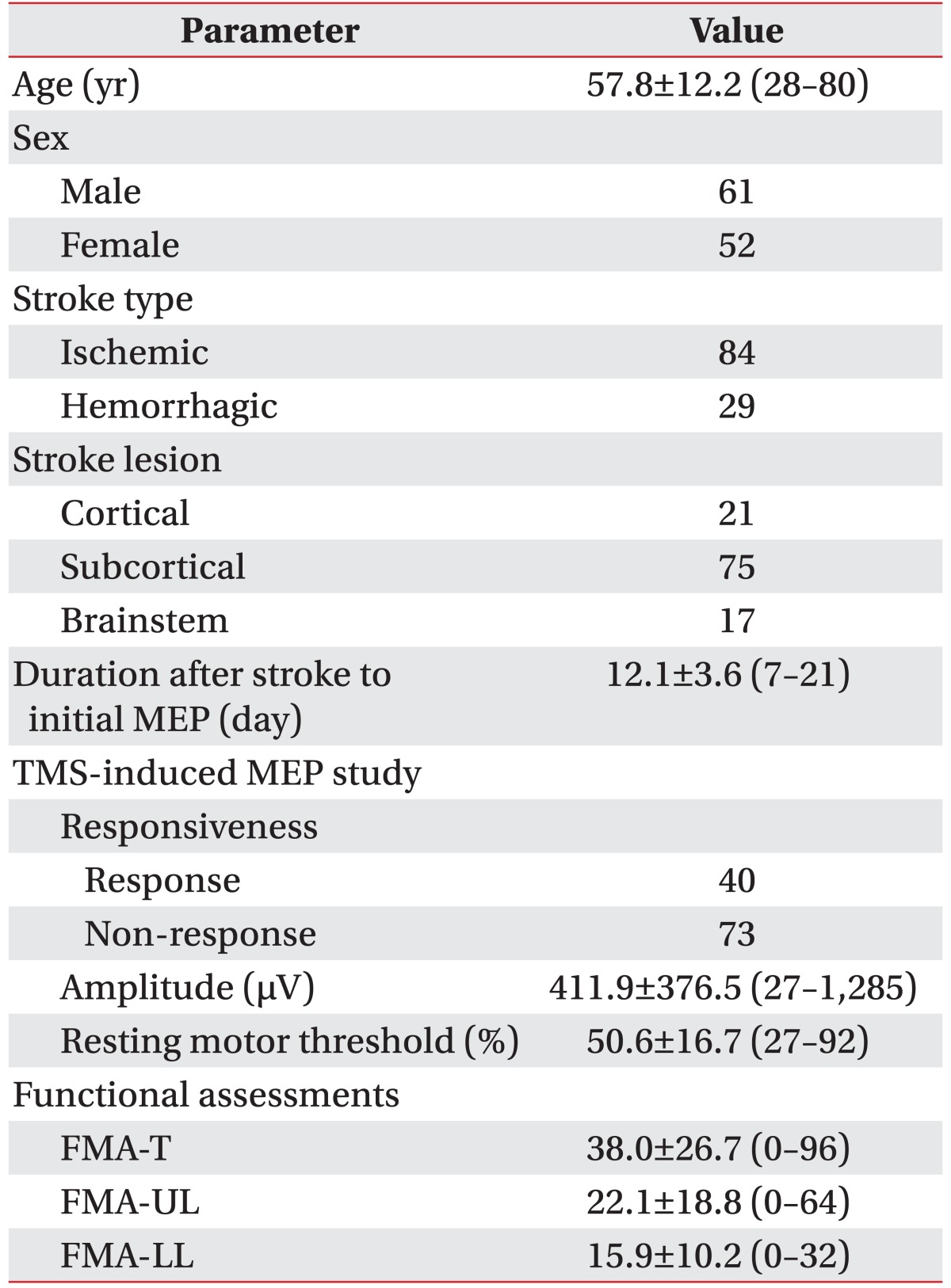
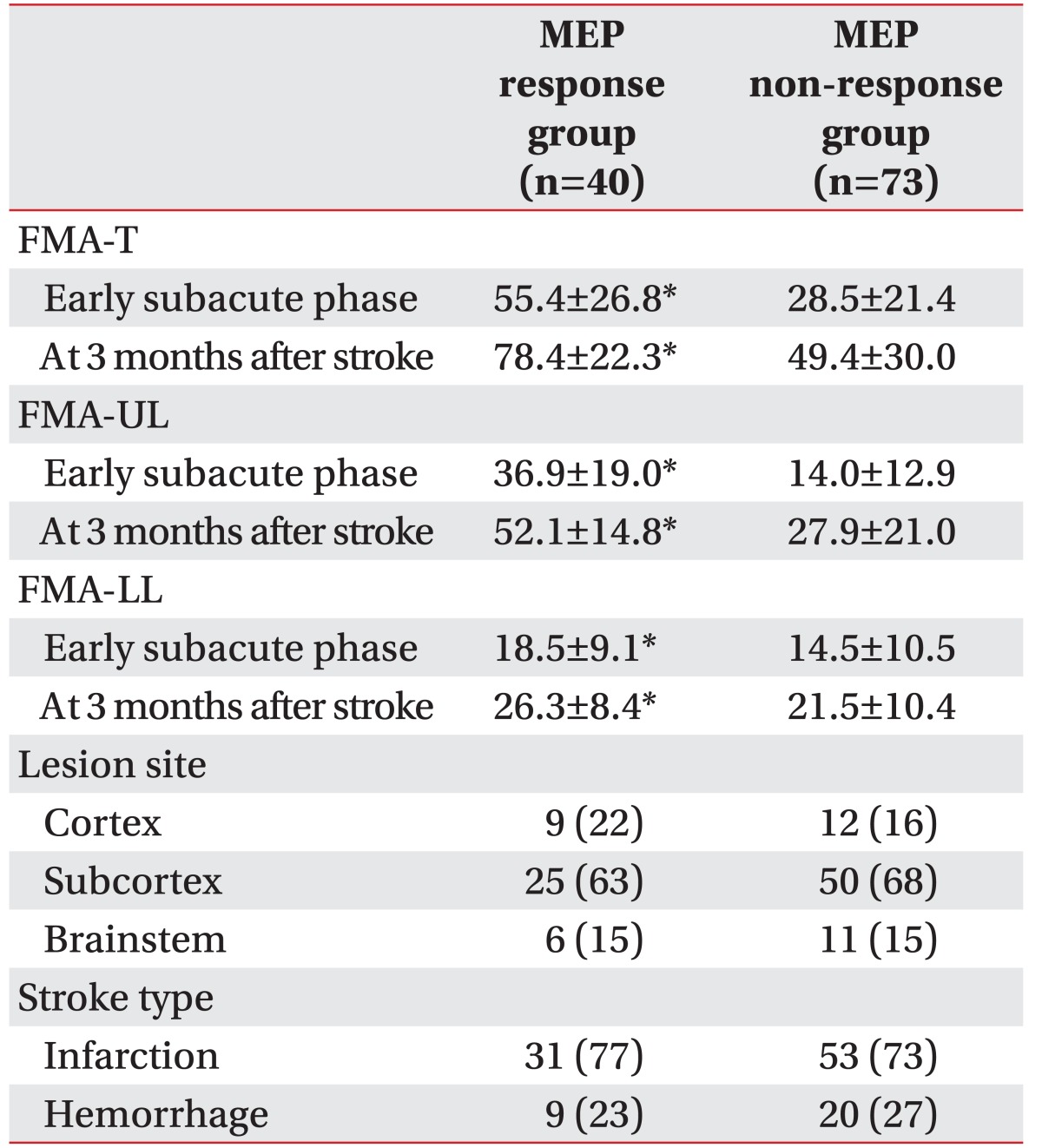
The clinical characteristics of patients are shown in Table 1. Of the 113 patients, 84 patients suffered an ischemic stroke and the other patients suffered a hemorrhagic stroke. With respect to the lesion location of stroke, 21, 75, and 17 patients were diagnosed as having cortical, subcortical, and brainstem lesions, respectively. After performing TMS-induced MEP, 40 patients and 73 patients were included in the MEP response group and the MEP non-response group, respectively. Comparison according to the responsiveness of MEP revealed that the FMA-T and FMA-UL were significantly higher in the MEP response group than in the MEP non-response group in both the early subacute phase and at 3 months after stroke onset (p<0.05) (Table 2).
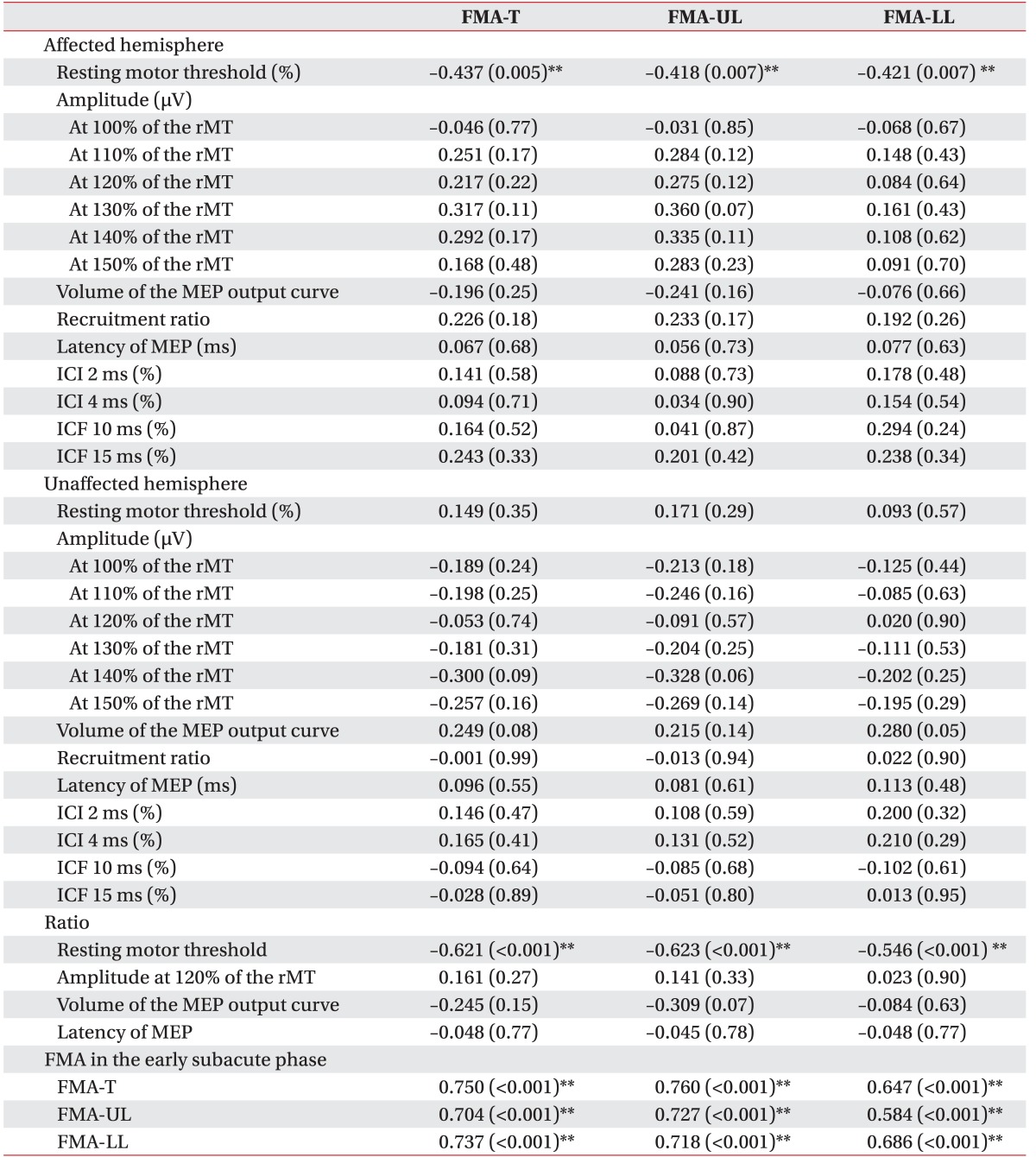
In the MEP response group, the mean MEP amplitude at 120% of the rMT was 411.9±376.5 µV and the mean rMT was 50.6±16.7 (Table 1). For the correlation analysis between MEP parameters and FMA score, in the affected hemisphere, the rMT showed negative relationships with FMA-T (Pearson coefficient=–0.437, p=0.005) and FMA-UL (Pearson coefficient=–0.418, p=0.007). The rMT ratio also showed a negative relationship with FMA-T (Pearson coefficient=–0.621, p<0.001) and FMA-UL (Pearson coefficient=–0.623, p<0.001). Other MEP parameters such as MEP amplitude at any intensity, volume of the MEP output curve, recruitment ratio, latency, ICI or ICF showed no significant relationship with motor function at 3 months after stroke. In addition, each FMA score in the early subacute phase after stroke onset showed a positive relationship with each FMA score at 3 months after stroke, respectively (Table 3).
In the multiple regression analysis, FMA score and rMT ratio, but not rMT in the early subacute phase were found to be independent prognostic factors for FMA-T (R2=0.633, p<0.001, F=0.011) and FMA-UL (R2=0.604, p<0.001, F=0.012) at 3 months after stroke (Table 4).
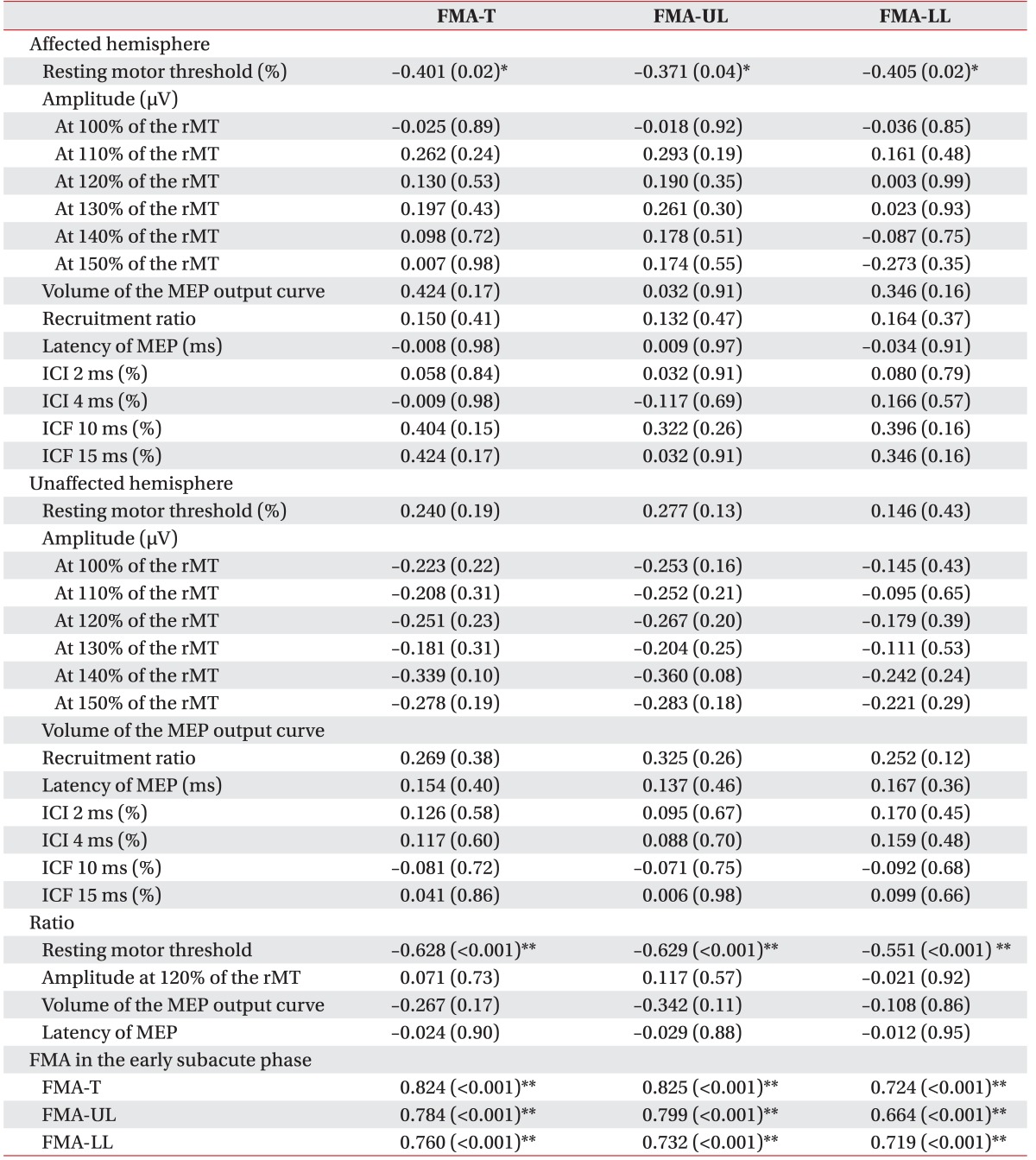
In the analysis according to the stroke type, the ischemic stroke group showed similar results. For the correlation analysis, the rMT in the affected hemisphere showed negative relationships with FMA-T (Pearson coefficient=–0.401, p=0.02) and FMA-UL (Pearson coefficient=–0.371, p=0.04). The rMT ratio also showed a negative relationship with FMA-T (Pearson coefficient=–0.628, p<0.001) and FMA-UL (Pearson coefficient=–0.629, p<0.001) (Table 5). However, multiple regression analysis revealed that the initial FMA score and rMT ratio, but not rMT were independent prognostic factors for FMA-T (R2=0.717, p<0.001, F=0.040) at 3 months after stroke. On the other hand, the hemorrhagic stroke group showed no relationship between MEP parameters and motor functional outcome. With respect to the stroke lesion classified as cortical, subcortical and brainstem, the result also showed no significant difference between each lesion site.
DISCUSSION
In the current study, we investigated the potential of TMS-induced MEP in the early subacute phase to predict motor function at 3 months after stroke onset. We could demonstrate two findings: (1) the MEP responsiveness was one of the strong tools to predict motor function at 3 months after stroke, (2) the rMT ratio in the early subacute phase was a significant independent prognostic factor for motor function at 3 months after stroke.
The MEP responsiveness as a parameter for predicting motor outcome was comparable with the results of previous studies [789101112]. MEP responsiveness showed high positive predictability of motor functional recovery compared to diffusion tensor tractography which showed high negative predictability [6]. Song et al. [12] reported that the low limit value of fractional anisotropy in the cerebral peduncle on the affected side was correlated with the poor hemiplegic limb motor function recovery in MEP non-responsive stroke patients because Wallerian degeneration of the cerebral peduncle occurred in accordance with changes in motor evoked potentials. However, there is no specific clue to reveal how MEP measures can be used as a predictive tool for motor recovery in MEP-responsive patients.
The results of this study revealed that the rMT and rMT ratio of MEP are significant tools for predicting motor functional outcome in MEP-responsive stroke patients. Furthermore, the multiple regression analysis revealed that rMT ratio in the early subacute phase was an independent prognostic factor for motor functional recovery. On the other hand, it showed no significant differences depending on the stroke type and lesion location, which could have been caused by the small number of patients. Motor function in the subacute phase is the strongest predictor for motor functional outcome in stroke patients [8]. rMT means threshold of the pyramidal tract responding to the magnetic stimulus which can reflect neuronal membrane excitability, thus a higher rMT ratio can be interpreted as an imbalance of motor threshold between bilateral primary motor cortices [2324]. In addition, Takechi et al. [25] showed that higher rMT may predict poor clinical recovery. In this context, this result suggests that the imbalance of motor threshold between bilateral primary motor cortices can be an important factor associated with late motor recovery. In stroke patients, neuronal excitability decreases, which leads to higher motor threshold in the affected side causing an imbalance of motor threshold [2026]. Furthermore, several studies postulated that the interhemispheric balance is disrupted in stroke patients and this caused suppression of ipsilesional cortical excitability by the contralesional hemisphere [272829]. Prashantha et al. [26] described that disruption of the transcallosal interaction could be the possible mechanism causing an imbalance of rMT. Considering these findings together, we can postulate that the patients with a higher rMT ratio may present lower cortical responsibility in the lesioned hemisphere, indicating lower cortical excitability. Therefore, it can be inferred that interhemispheric inhibition could be the possible mechanism of imbalance of bilateral hemispheres, interfering with motor recovery in stroke patients. In other words, the contralesional hemisphere may provide more suppression via the transcallosal inhibitory circuit, and consequently inhibit the recovery of ipsilesional motor cortical function.
With respect to the other MEP parameters such as amplitude or latency as prediction tools for motor recovery, several studies reported on the amplitude or amplitude ratio of MEP and they showed incongruent results [910]. Choi et al. [9] indicated that MEP responsiveness and amplitude ratio are significantly associated with the upper extremity function evaluated by Brunnstrom stage of hand recovery and the Modified Barthel Index at the time of admission. However, in this study, we could not reproduce the relationship between amplitude or amplitude ratio of MEP and motor functional outcome such as FMA scores. Kim et al. [10] also indicated that MEP responsiveness and amplitude ratio are significantly correlated with the MRC scale and the Modified Barthel Index. However, both these studies investigated the correlation between MEP parameters and motor function and both studies assessed patients in the subacute stage of stroke, which was different from the present study which investigated long-term functional outcomes. In addition, considering that the amplitude of MEP represents the corticospinal excitability of the M1 [23], it can be affected by temporal dispersion of corticospinal fiber tract conduction, which can confound the results [23]. In addition, the amplitude of MEP can be influenced by other contributing factors such as height or status of peripheral nerves and muscles [30]. Moreover, amplitude of MEP in the affected hemisphere may not represent the absolute value of cortical excitability. The latency of MEP might be influenced by peripheral nerve conduction time as well as central conduction time [23]. Because cortical motor output is the net result of the interplay between multiple systems that exert excitatory or inhibitory influences on the corticospinal neurons, ICI and ICF could represent intrinsic intracortical connectivity and cortical plasticity. ICI is suppressed on the affected side in the first few weeks after the ictus [15273132], whereas ICF is consistently normal [273132]. This suggests that the balance of excitability in intracortical circuits shifts towards excitation. Whether the reduction of ICI relates to the degree of disability is rather controversial [3132]. Several studies showed that interventions such as motor task training, active or passive training, transcranial direct current stimulation could be related to reduced ICI, thus facilitating motor recovery [2225333435363738]. However, the exact mechanism and causality of the correlation remain unclear and interpretation of ICI and ICF is complicated because they could be affected by various factors like position, intensity of test stimulus, and medication [3940]. Taking all these aspects together, we can postulate that the rMT ratio may better reflect the changes in the motor cortical excitability after stroke than the other parameters of MEP.
This study has some limitations. First, this study retrospectively analyzes the patients who were transferred to our hospital and underwent inpatient rehabilitation therapy after stroke; therefore, there may be a bias of analyzing significantly affected patients. Second, the initial time period for obtaining first MEP data is rather variable, ranging from 1 to 3 weeks after stroke. Finally, the present study cannot identify whether stroke type or lesion location could affect the relationship between MEP parameters and motor functional outcomes. Clinical recovery after stroke depends on the ability to activate intrinsic cortical connections in the most efficient manner as well as the activation of corticospinal excitability itself. Some insight into the mechanisms of recovery in these individuals could be provided by more complex TMS measures that examine function of the intrinsic cortical pathways. Therefore, prospective investigations are required in future to overcome these limitations and to obtain a better predictive value of MEP parameters for motor recovery after stroke.
In addition to the responsiveness of MEP being an important factor for predicting motor function, the rMT ratio in the early subacute phase was also significantly correlated with motor recovery of the upper limb at 3 months after stroke onset. The quantitative measure of TMS-induced MEP could be used as a parameter to predict motor recovery in patients with stroke.

 XML Download
XML Download