

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ankle ligament injury is a common trauma that occurs during sports activities, and accounts for over 40% of all exercise-related ailments; it most frequently occurs in sports such as basketball, soccer, running, ballet, and dancing [1,2].
Most ankle ligament injuries are caused by sudden flexion and inversion of the ankle joint, which impairs the lateral ligamentous structure. Due to the tendency for ankle ligament injuries to recur, patients tend to experience this injury repeatedly. Such repeated inversion injury can cause chronic ankle instability [2-5].
There are two major causes of chronic ankle instability. One is mechanical instability caused by structural loss of ligaments around the ankle after an injury, which becomes a risk factor for recurrent ankle injury, as the range of joint motion becomes abnormal [6]. The other one is functional instability, which is caused by loss of neuromuscular control after injury. Freeman [7] mentioned functional instability as a cause of recurrent ankle injury in his report on the impaired balancing ability of patients with ankle injury while standing on one foot (unilateral stance). Afterwards, many studies reported the reduction of balancing ability [8,9] and proprioception [10-15] in patients with chronic ankle instability.
However, various treatments have been introduced due to the high incidence of ankle ligament injury and functional instability. So far, the primary ones have been ligament reconstruction surgery with various methods, and functional rehabilitation exercises. Functional rehabilitation exercises that include balance training are focused on recovery from functional instability of the ankle joint, which can occur after an ankle injury, using the following mechanisms: muscle strengthening and improvement of neuromuscular control; proprioception enhancement; balancing ability enhancement; and posture control ability enhancement for ankle muscles including the peroneal muscle, a lateral dynamic stabilization structure of the ankle. As a matter of fact, the effects of such therapies have been proven in studies by McKeon et al. [16] and O'Driscoll et al. [17] In addition, various taping or bracing methods that directly support the lateral ankle ligament are in use [18].
Several recent studies reported that application of ankle-foot orthosis to patients with chronic ankle instability led to enhancement of static balance ability [10] and increased ability to control posture [19]. There is also a study that demonstrated improvement in kinematics and dynamics of ankle joints after application of foot orthotics [20]. However, there are no studies demonstrating the effects of foot orthotics with respect to functional movements as apposed to the static stance such as standing and simple linear walking.
Therefore, this study compared and analyzed the changes in the balancing abilities of athletes with chronic ankle instability who were engaged in a functional rehabilitation exercise program for which patients had to use their proprioception sense, and exercise their static and dynamic balance abilities, or who were engaged in doing functional movements while wearing foot orthotics.
MATERIALS AND METHODS
Objectives
The research was done by dividing 50 male athletes, who received sports rehabilitation treatment for ankle instability from February 2010 to July 2011 at our hospital, into two groups: the 'ankle rehabilitation exercise treatment group' and the 'foot orthotics application group'. The subjects were assigned into the two groups in the order of their participation. The rehabilitation exercise treatment group had existing balancing ability enhancement training and neuromuscular control exercises, and the foot orthotics application group used foot orthotics during their rehabilitation exercises. The subjects were patients with chronic ankle instability after suffering from repeated ankle injury, and had chronic pain and instability after being inflicted with an inversion ankle injury of at least a moderate level several years previously. However, patients inflicted with pelvic limb fractures or other joint injuries within 3 months after participation or those unable to perform functional movements such as running due to edema of at least a moderate level on their ankle were excluded. During the first test, biomechanical assessment of the foot and assessment of ankle proprioception and balance were conducted.
Methods
Rehabilitation treatment method
All participants received rehabilitation exercise therapy for an hour a day, 3 days a week over 4 weeks. Rehabilitation exercises included balancing ability enhancement training and neuromuscular control exercises. From the first week, joint mobilization exercises that depended on weight-bearing and isotonicity, and isometric strength training were carried out, along with balancing ability enhancement training on a balance board and trampoline. During the latter part of training, plyometrics training and agility training were added to the rehabilitation exercises.
Foot orthotics application
The angle between the forefoot to the rearfoot and the resting calcaneal stance position angle were measured during a biomechanical assessment of the foot [21]. The forefoot to rearfoot angle was the angle formed by two blades of a protractor when the tester grabbed the mediolateral part of the upper talus with a thumb and an index finger, to maintain the neutral position of the lower talus ligament while one of the blades was positioned along the condyle and the other blade was placed parallel to the calcaneus dichotomization line. The resting calcaneal stance position angle is the angle formed between the calcaneus dichotomization line and a vertical line when the patient naturally marched in place and stopped. Based on the test, the shapes of the foot were categorized into the following 3 types: pronated foot, erect foot, and supinated foot. Pronated foot applied to the resting calcaneal stance position angle of -3 degrees or lower or a forefoot to rearfoot angle with inversion of 3 degrees or higher. Supinated foot applied to the resting calcaneal stance position angle of +3 degrees or higher or a forefoot to rearfoot angle with eversion of 3 degrees or higher. Meanwhile, erect foot referred to a status in between pronation and supination of the foot.
Based on these three types, foot orthotics were prescribed and applied to each patient perpendicular to foot location (forefoot to rearfoot angle upon standing) according to their foot type. For the pronated foot, TPScan (BioMechanics, Goyang, Korea) H type off-the-shelf ankle-foot orthosis that used large arch support technology and inner heel wedge technology was applied, and an arch support (made of ethylene-vinyl acetate [EVA] material) and inner heel wedge were added until the resting calcaneal stance position angle reached between 0 and -2 degrees. For the erect foot, TPScan P type orthosis with only a little bit of arch support technology was used and a wedge in the shape of a half-dome was attached to the lower lateral part of the calcaneocuboid joint to prevent the rearfoot from turning laterally. The function of the wedge is to give sensory stimulation to the skin below the calcaneocuboid joint. If a foot gets pushed or overturned laterally, the wedge sends sensory feedback by applying pressure to the skin below the calcaneocuboid joint. For the supinated foot, lateral forefoot wedge technology at a moderate level and TPScan S type orthotics with half-dome wedge technology to the lower part of the calcaneocuboid joint was used. In addition, a lateral forefoot wedge or lateral rearfoot wedge was used to make the resting calcaneal stance position angle reach between 0 and +2 degrees.
Proprioception assessment
Joint reposition sense testing was used to assess proprioception, along with the CYBEX 770 system (CYBEX, Medway, MA, USA), a constant exercise equipment (Fig. 1). All subjects wore blindfolds and earplugs to block their visual and auditory senses, and sat at an iso-inclination of 70 degrees with their knee flexed at an angle of 60 degrees, while their feet and ankles were diagonally wrapped with tie-downs that were fixed to the equipment footsteps. The active inversion of the ankle and range of joint motion of eversion were measured prior to the joint reposition sense test. Then, a target angle was individually set after setting the joint location at 25% and 75% of the maximum range of joint motion of each subject. This was done to avoid reaching the end range of joint motion in order to minimize additional sensory stimulation from skin sensory receptors [22]. The tester had each subject recognize the target angle passively, pause for 10 seconds and move their ankles passively at a neutral angle. Afterwards, the subjects were asked to move their ankles at the target angle they recognized and were given a stop signal when they seemed to reach the target angle. Three tests were performed to measure the errors in reference to the target angle and three averages were used as data.
Balancing ability
For balancing ability assessment, the Balance Master system (NeuroCom Inc., Clackamas, OR, USA) was used for the following three areas of assessment: sensory limitation assessment of static balancing ability; motor limitation assessment of dynamic balancing ability; and functional limitation assessment of motor functions.
Sensory impairment assessment for static balancing ability: Balancing ability assessment included the follow-ing 3 items: percentage of weight-bearing on both pelvic limbs, Modified Clinical Test Sensory Interaction on Balance (mCTSIB), and unilateral stance. The percentage of weight-bearing test calculated the percentage of weight-bearing on both pelvic limbs while the subject stood on the force plate at a knee angle of 0, 30, and 60 degrees. mCTSIB measured the center of gravity (COG) sway velocity (/sec) by having the subjects stand on a foam box or another soft object that was placed on the force plate, which would confuse their sense of proprioception, for 10 seconds with their eyes open and another 10 seconds with their eyes closed (Fig. 2). The unilateral stance test assessed the COG sway velocity by having the subjects stand on the force plate with one foot for 10 seconds with their eyes open and another 10 seconds with their eyes closed. Each test was repeated three times to obtain the average value (Fig. 3).
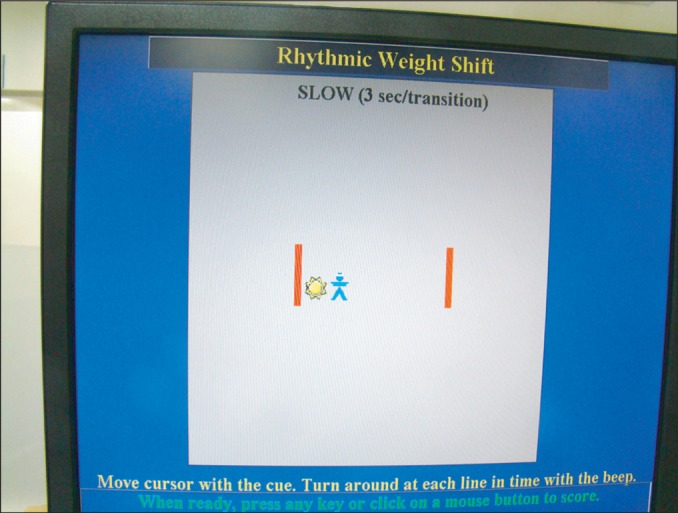
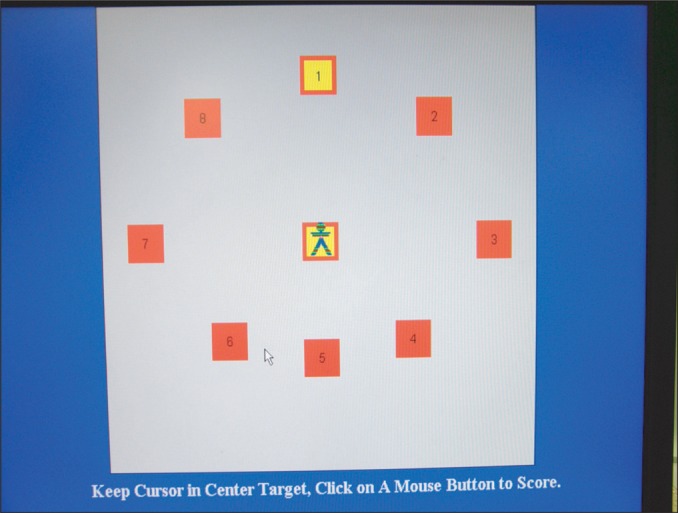
Motor impairment assessment for dynamic balancing ability: The motor impairment assessment measured the following two items: rhythmic weight shift and limits of stability. Rhythmic weight shift test measured the on-axis velocity (/sec) and directional control (%) of the COG by having the subjects actively move the COG in all directions (Fig. 4). The limits of stability test tests how far the subjects can intentionally move their COG in all directions and the maximum excursion is measured in this test (Fig. 5). Each test was repeated three times to obtain the average value.
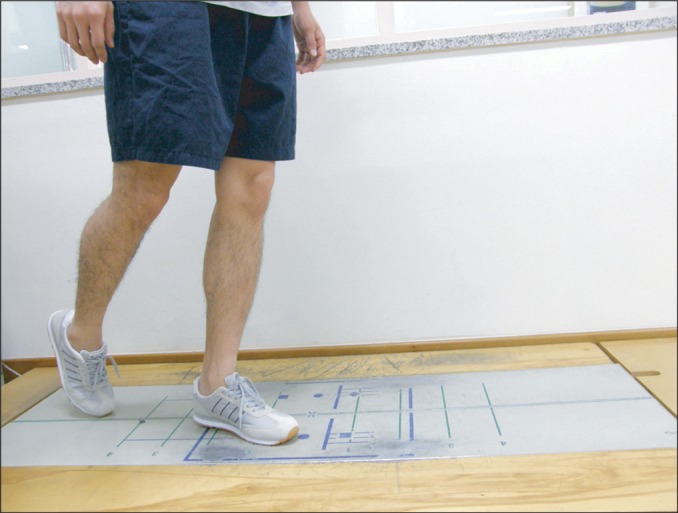
Motor impairment assessment for functional movements: This assessment includes the following three items: changing direction (step/quick turn), stepping over an obstacle (step up/over), and taking a big step forward (forward lunge). The step/quick turn test was done as follows. The subjects at the starting point took two steps with one foot on the force plate at the testers' command to start and they changed their direction by 180 degrees to return to the starting point (Fig. 6). The COG sway velocity and the time they took to change their direction (/sec) were measured. The step up/over test was done by having the subjects climb onto a hard obstacle that was 20 cm tall with one foot on the force plate and then step over the obstacle with the other foot (Fig. 7). The lift-up index that indicates the power that lifts the body in the vertical direction, the movement time, and the impact index that indicates the power of a step applied to the force plate in the vertical direction were measured as a proportion (%) of the weight. The forward lunge test was done as follows. The subjects at the starting point took a big step forward with one foot at the tester's command to start and then returned to their original place (Fig. 8); this test was done with each foot alternating. The test measured the following: % distance, which indicates the distance of steps as the COG moves as a proportion of the height; impact index, which indicates the maximum power applied to the force plate; contact time, which is the time that a step is in contact with the force plate; and force impulse, which is the total power of a step applied to the force plate. Each test was repeated three times to obtain the average value.
Analysis
SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis of the study. All data were shown as average values and standard deviations. An independent t-test was done to compare the differences in the measured values between the exercise treatment group and the foot orthotics application group. A paired t-test was done to compare the differences in the measured values before and after assessment of each group. Modified Bonferroni was used for multiple comparisons, and p-values for statistical verification were set at below 0.05.
RESULTS
General characteristics of subjects
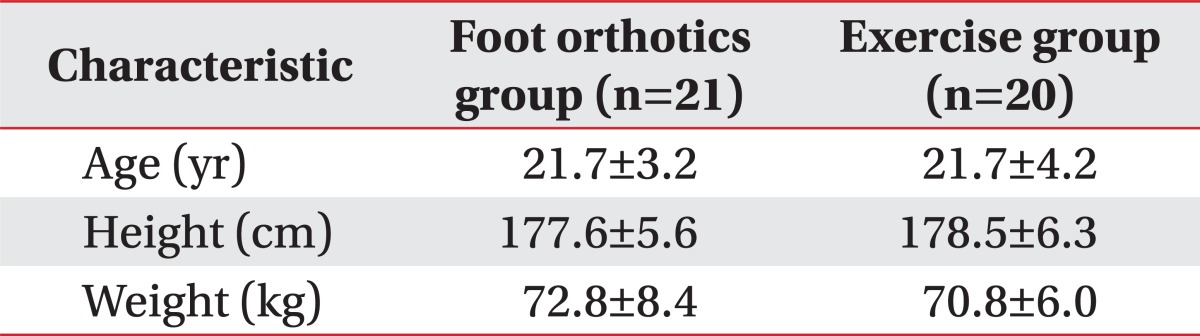
Forty-one out of 50 athletes completed the 4-week long study. They were all males with ages between 17 and 32. There were 18 athletes with instability of the left ankle, 20 with instability of the right ankle, and 3 with instability of both ankles. In terms of sports played, 36 were soccer players, 3 were volleyball players, 1 was a tennis player, and 1 was a judo athlete. The foot orthotics application group had 21 subjects including 10 with pronated foot, 5 with supinated foot, and 5 with erect foot (affected foot). The rehabilitation exercise treatment group had 20 subjects including 5 with pronated foot, 4 with supinated foot, and 11 with erect foot. The average age of both groups was 21.7 years. The average height of the foot orthotics application group was 177.6 cm and the average weight was 72.8 kg. The average height of the rehabilitation exercise treatment group was 178.5 cm and the average weight was 70.8 kg (Table 1).
Proprioception assessment
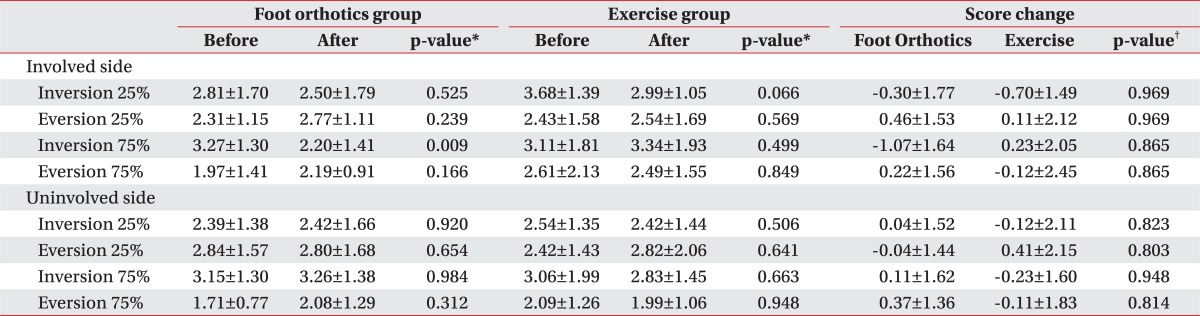
The joint reposition sense test (error values) conducted for proprioception assessment showed the following results. The affected foot's eversion 75% angle assessment of the foot orthotics application group was significantly reduced from 3.27±1.3 degrees before treatment to 2.20±1.41 degrees after treatment with an average change of -1.07±1.64 degrees. On the other hand, the same assessment of the rehabilitation exercise treatment group showed no significant differences; this group went from 3.11±1.81 degrees before treatment to 3.34±1.93 degrees after treatment, with an average change of 0.23±2.05 degrees. Although the foot orthotics application group showed greater improvements, there were no statistically significant differences between the two groups. Meanwhile, inversion 25%, eversion 25%, and inversion 75% of the affected foot and unaffected foot showed no statistical differences when the before and after treatment in each group and the degree of improvement between the two groups were compared (Table 2).
Sensory impairment assessment on static balancing ability
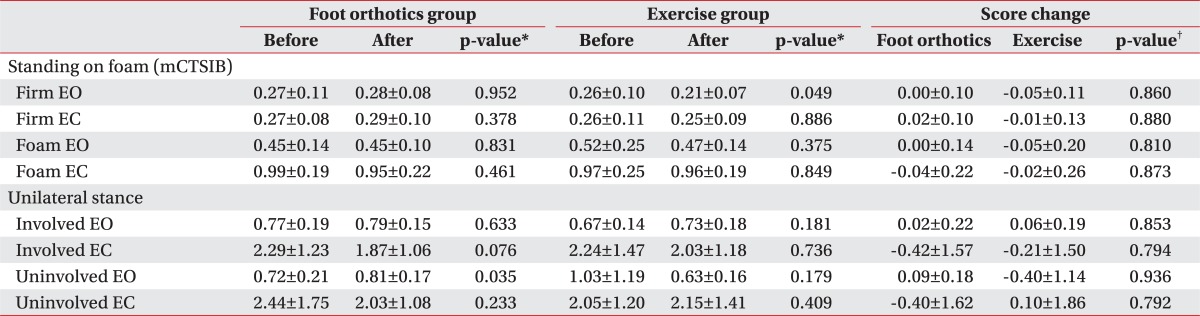
The test that assesses the percentage of weight-bearing on both pelvic limbs showed no predominance of either the affected or unaffected foot at 0°, squat30°, squat60°, and squat90° in both groups. During the mCTSIB test done on the force plate with the eyes open, the COG sway velocity was reduced by 0.00±0.10 in the foot orthotics application group and by 0.05±0.11 in the rehabilitation exercise treatment group, suggesting that the latter group showed greater improvement, although there was no statistical significance in both groups. Meanwhile, COG sway velocity measured on a soft foam box with the eyes closed was reduced by 0.04±0.22 in the foot orthotics application group and by 0.02±0.26 in the rehabilitation exercise treatment group, indicating that there were no significant differences between them. Also, there were no statistical differences in the sway test done by standing on the force plate with one foot for 10 seconds (Table 3).
Motor impairment assessment on dynamic balancing ability
The rhythmic weight shift test that involved movement of the COG in all directions showed no statistical differences between the two groups in terms of on-axis velocity with three different transfer speeds and directional control of COG. In the limits of stability test where the COG was moved to a maximum level in every direction, the maximum excursion (rear) of the COG on the affected foot was reduced by 4.71±7.95 in the foot orthotics application group and increased by 3.65±12.40 in the rehabilitation exercise treatment group, with no statistical significance within both groups (Table 4).
Motor impairment assessment on motor functions
In the step/quick turn test at 180 degrees, one of the functional limitation assessment items, the time of changing direction by the affected foot declined by 0.04±0.24 seconds in the foot orthotics application group and by 0.20±0.20 seconds in the rehabilitation exercise treatment group, with no significant differences between the two. In the COG sway test, COG rose by 0.07±5.31 in the foot orthotics application group and declined by 3.15±4.50 in the rehabilitation exercise treatment group, with no statistical differences between them (Table 5). In the step up/over test, although the lift-up index that indicates the power of lifting the body in a vertical direction improved by 3.82%±7.96% in the foot orthotics application group and by 6.95%±11.01% in the rehabilitation exercise treatment group, there were no statistical differences. In the forward lunge test, the time of contact of the affected foot with the force plate decreased by 0.08±0.13 seconds in the foot orthotics application group and by 0.06±0.19 seconds in the rehabilitation exercise treatment group, showing no statistical significance between the groups.
DISCUSSION
The reduction in proprioception of patients with chronic ankle instability is known to be caused by blockage of afferent nerve fibers of mechanoreceptors located on the articular capsule and ligament of the ankle, due to chronic injury or instability of the ankle [10-15].
According to existing studies, foot orthotics that involves applying a lateral wedge to the feet of patients with chronic ankle instability increases pronation of the hindfoot and controls the lateral movement of the ground reaction force while the foot is on the ground, preventing re-injury such as an inversion ankle sprain [20]. In addition, Feuerbach et al. [14] reported that application of ankle-foot orthosis improves the position sense because of an increase in the afferent sensory feedback from skin receptors.
Also in this study, improvement in proprioception was expected to occur with an increase in afferent signals delivered to the mechanoreceptors or skin receptors of the ankle when the biomechanical position of a normal ankle was simulated through application of individual ankle-foot orthosis that induce neutral position of the hindfoot and forefoot, based on biomechanical analysis of the foot and ankle of athletes who participated in the experiment. In addition, stabilizing the ankle, improving posture control ability, and helping to maintain the dynamic balance and establishing a normal balance by limiting the compensation of the knee and pelvic limb were expected. Guskiewicz and Perrin [23], who compared the balancing ability of young athletes inflicted with an acute ankle ligament injury after they were divided into a foot orthotics application group and a group without foot orthotics, reported that the foot orthotics application group showed improvement in their balancing ability. In addition, Stude and Brink [24] demonstrated that professional golfers who used ankle-foot orthosis for 6 weeks experienced significant improvement in their proprioception and balancing abilities. Cobb et al. [25] reported that 6-week application of ankle-foot orthosis to patients with forefoot varus deformity led to a dramatic improvement in their posture stability.
In this study, however, the comparison of a group that had both ankle rehabilitation exercises and foot orthotics and another group with only ankle rehabilitation exercise treatment found no statistical differences between them in terms of static balance, dynamic balance, and balancing ability for functional movements. The reason that application of foot orthotics was not very effective in this study, unlike in others, is probably due to the following differences. First, there was a difference in foot orthotics application status during the reassessment. While other studies reassessed the balancing ability while the patient was wearing foot orthotics after using it for several weeks, this study performed the reassessment after removal of the foot orthotics. This was done because many studies have already demonstrated improvement in balancing ability when the subject is wearing foot orthotics, but there were almost no studies that assessed the balancing ability after removal of the foot orthotics. Second, the ankle rehabilitation training was probably a highly influential confounding factor. Existing studies demonstrated improvement in the balancing ability of most adults as well as athletes with rehabilitation exercise treatment. McKeon et al. [16] reported improvement in the static balance and dynamic balance abilities of patients with chronic ankle instability with rehabilitation exercise treatment involving 4-week balance training. In addition, O'Driscoll et al. [17] demonstrated improvement in balance and functions of the ankle joint of athletes with ankle instability through 6-week dynamic neuromuscular control training.
In this study, functional rehabilitation exercises that included proprioception enhancement and balancing ability enhancement training were applied to both the group that used foot orthotics and the other group that did not. This is because all the athletes in both groups were patients in need of therapeutic interventions such as rehabilitation exercises. Because rehabilitation exercises were a highly influential confounding factor, this was probably the reason for the lack of differences between the two groups.
Meanwhile, the reason that the rehabilitation exercise treatment group showed improvement in only a few items, rather than overall improvement across all items, after treatment is probably due to the following. In this study, athletes underwent a 4-week rehabilitation program. Although the content of the program was adequate compared to other studies, the training was not executed every single day, unlike in other studies. In addition, even though participation and compliance are crucial in a rehabilitation program, the patients in this study were not continuously managed. In fact, since the subjects simultaneously participated in the main training of their teams, this is likely to have led to rehabilitation exercises showing less beneficial effects. Therefore, assessing the effects of treatment is necessary through another rehabilitation exercise program that overcomes such limitations in future studies.
This study has two important implications. First, by comparing the effects of foot orthotics application on a wider variety of dynamic postures including postures involving changes of direction of 180 degrees and stepping over an obstacle, rather than only static postures or walking straight, it presents a novel investigation. Second, this study proved that the beneficial effects of foot orthotics decrease once the orthotics device is removed even after it has been used for several weeks, leaving only the positive effects of ankle rehabilitation exercises.
As for limitations of this study, the subjects were all young male athletes, making it difficult to generalize the results to the general public, and the number of subjects was fairly small. Therefore, similar studies with no such limitations should be carried out. In addition, although subjects with each of the three foot types (pronated foot, supinated foot, and erect foot) should be assigned to the groups in equal numbers, the foot orthotics application group had more patients with a deformity (pronated foot or supinated foot), which could have affected the results. Thus, future studies should be carried out with unified foot types.
Since having an intact proprioception sense and good balancing ability of the ankle joint are crucial factors in preventing injury, proper therapeutic intervention for athletes with ankle instability is essential. This study demonstrated that when foot orthotics is removed after 4 weeks use in a patient who received ankle rehabilitation exercise treatment, orthotics did not offer any additional benefits, although it provided the proper biomechanical environment of the ankle and increased plantar skin sensory signals.







 XML Download
XML Download