

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Approximately one third of stroke patients suffer from dysphagia, and are prone to complications such as malnutrition, aspiration pneumonia and dehydration.1 According to an evaluation with a video fluoroscopic swallowing study, the incidence of aspiration for acute stroke patients is reported to range from 21-51%, and reduces to 12% after three months.2 Dysphagia can occur with all stroke types involving the cerebrum, cerebellum and brainstem. The cerebrum engages in the migration of a bolus and mastication. A stroke involving the precentral gyrus can especially deteriorate the accommodation of movements in the face, lips and tongue, and the peristaltic movement of the pharynx.3 Brainstem lesions cause decreased sensations of the tongue and oral cavity, and deterioration of its function related to initiating the pharyngeal phase during the swallowing process, leading to more severe dysphagia.3,4 Dysphagia is not only caused by a disease of the central nervous system such as stroke, but also by structural problems such as diverticulim, and psychiatric disorders.5 Therefore, even in cases of dysphagia caused by a stroke, diverse factors must be taken into consideration if improvements are not present over time.
A retropharyngeal abscess mostly develops in pediatric patients and rarely occurs in adults.6 The occurrence of a retropharyngeal abscess in adult patients is commonly accompanied by an immunocompromised status, preceding trauma or infection.7 Expectable symptoms include cervical pain, dysphagia, sore throat and on rare occasion, upper airway obstruction.7
In this case, there were no improvements of dysphagia after ten weeks following a hemorrhagic stroke. The cervical pain was associated and the patient was on the treatment of diabetes mellitus diagnosed during an admission period after the onset of subarachnoid hemorrhage. On evaluation with a video fluoroscopic swallowing study, the retropharyngeal abscess was identified. Treatment with antibiotics was performed and lead to a decrease in the dysphagia and cervical pain.
CASE REPORT
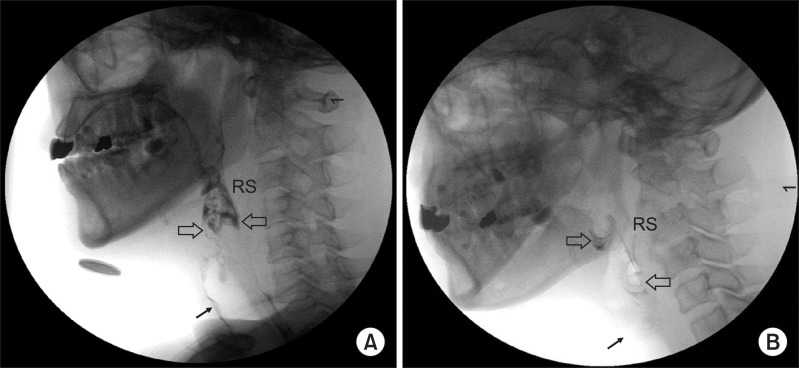
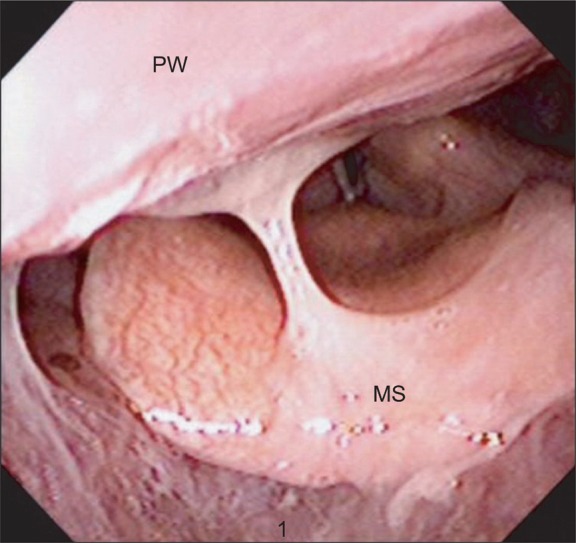
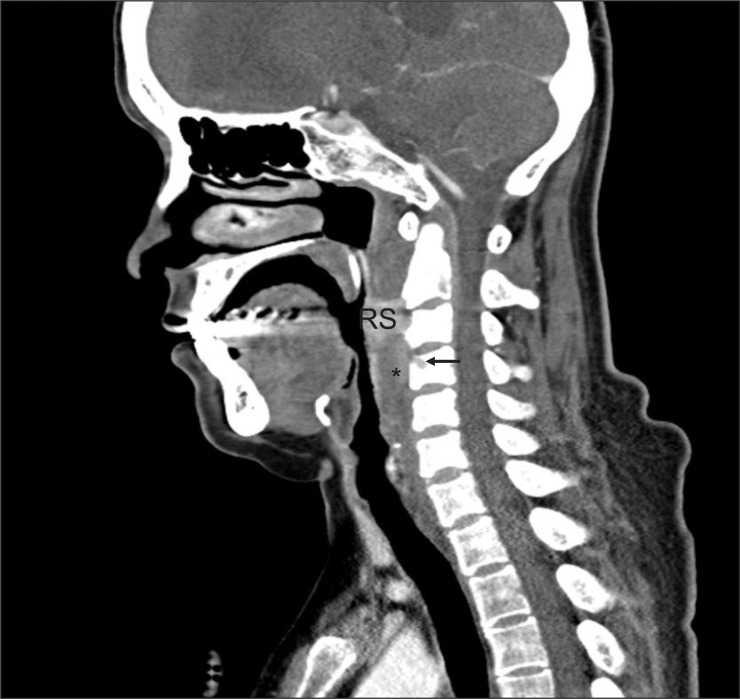
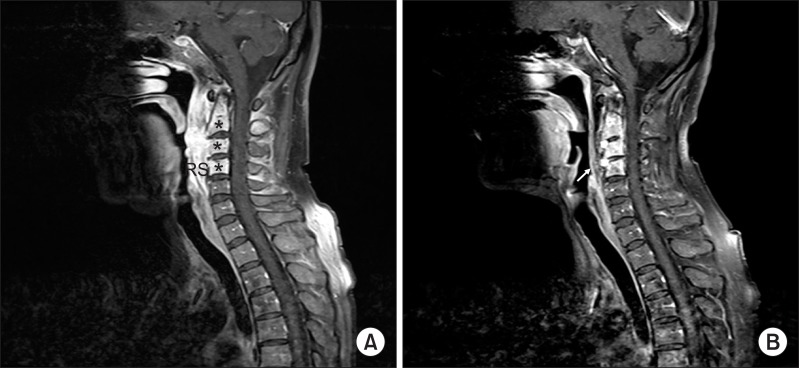
A 49-year old female patient was admitted to the department of neurosurgery at another hospital under the diagnosis of a subarachnoid hemorrhage. She underwent a decompressive craniectomy, surgical neck clipping of ruptured aneurysm and hematoma removal. The patient was treated in the intensive care unit for three weeks. The patient had no prior operative history of tracheostomy, and a cranioplasty was performed. Following the completion of intensive care, the patient was moved to a general ward, and transferred to the department of rehabilitation medicine. At the time of the transfer, the patient was alert and conscious with motor power in the right upper and lower extremities that presented at a grade one on examination. To independently turn-over in bed was possible, but sitting-up required moderate assistance. The patient showed difficulty in maintaining balance while seated and generally required moderate assistance in daily activities. The patient was on Levin tube feeding, and treatment for dysphagia was carried out. The patient was transferred to our department of rehabilitation medicine at ten weeks after the onset of a hemorrhagic stroke. On admission to our hospital, the patient presented with persistent dysphagia, and was still receiving Levin tube feeding. Cervical pain with severity of grade four to five according to visual analogue scale was rated by the patient. The exact onset of diabetes mellitus was uncertain but HbA1c was 5.5% on laboratory examination, and the patient had no family history of diabetes mellitus. The patient was on insulin therapy, but the medication regimen was modified to the administration of Metformin Hydrochloride 500 mg two times a day owing to adequate control of blood glucose level, and afterward, the patient had a favorable blood glucose level. The vital signs were stable on admission with a blood pressure at 106/73 mmHg, heart rate 98/minute, respiratory rate 19/minute and body temperature of 36.3℃, and the patient did not present with respiratory distress. Motor power examination showed normal findings on the left side, but the right upper extremity presented with a grade one and the right lower extremity presented with grade two. Her cognitive function was rated with score of 22 according to Korean Mini-Mental State Examination (K-MMSE). Blood test results showed no remarkable abnormal findings other than a mildly elevated ESR level of ESR 36 mm/hr. Other results revealed WBC 8,410/µl and CRP 0.04 mg/dl. On a video fluoroscopy swallowing test for the evaluation of dysphagia, retropharyngeal edema was identified, which lead to impairment of a migration of bolus into the esophagus, and the aspiration occurred due to residual contents (Fig. 1-A). With a consultation to the department of otolaryngology, a laryngoscopy was performed and retropharyngeal edema and profuse discharge were identified (Fig. 2). A cervical computed tomography examination showed generalized retropharyngeal edema and cortical contrast enhancement of the fourth cervical spine along with partial osteoclastic findings (Fig. 3). An additional differential diagnosis of retropharyngeal abscess, malignant tumor and tuberculous spondylitis, cervical magnetic resonance imaging (MRI) was carried out, and revealed a signal change at the medulla from the second to the fourth cervical spine along with generalized retropharyngeal edema. At the anterior portion of the second to fourth cervical spine, a soft tissue lesion of low signal intensity on T1, high signal intensity on T2, and contrast enhancement was identified (Fig. 4-A). The marginal portion of the abscess did not show contrast enhancement, and the posterior portion of the vertebral body adjacent to the retropharyngeal space showed contrast enhancement. This lead to difficulty in excluding the malignant tumor, and a biopsy was planned. The location of the lesion was difficult to access for complete resection or incision and drainage. Since the trial of the incision and drainage does not affect the period of antibiotics administration, an excisional biopsy under local anesthesia was performed, and an acid-fast bacillus stain along with a culture study was carried out. Biopsy results revealed findings consistent with inflammatory granulation tissue and acid-fast bacillus staining which showed no specific findings. A culture study showed positive results for Staphylococcus aureus susceptible to methicillin. The lesion was concluded as a retropharyngeal abscess, and treatment with antibiotics was initiated with the administration of intravenous Cefazolin 2 g every 8 hours. The total treatment period with antibiotics was eight weeks. The follow-up evaluation with blood tests showed no abnormal findings regarding the WBC, ESR and CRP. Re-evaluation with cervical MRI after treatment with antibiotics showed improvement of a retropharyngeal abscess (Fig. 4-B). On video fluoroscopic swallowing study, aspiration was not observed, and the residual contents were remarkably decreased leading to initiation of feeding with a regular diet (Fig. 1-B). The cervical pain was managed with the administration of Tramadol HCL 18.75 mg/Acetaminophen 162.5 mg three times a day since admission but did not show improvement. However, the cervical pain started improving after the initiation of treatment with intravenous antibiotics. Medication with Tramadol HCL 18.75 mg/Acetaminophen 162.5 mg was administrated for a total period of four weeks, and the patient no longer complained of cervical pain.
DISCUSSION
Dysphagia is a common finding for patients being treated at rehabilitation facilities. Diseases of the central nervous system including stroke, Parkinson's disease and traumatic head injury are well-known causes of dysphagia.8 Other causes include structural lesions such as: a tumor, Zenker's diverticulum, congenital laryngeal web and thyroid hyperplasia, psychological problems, fibrosis due to radiation, and surgery involving the head and neck.5 In one study regarding the incidence of aspiration in acute stage stroke patients, an evaluation with a video fluoroscopic swallowing study showed aspiration in 51% of patients directly after the onset, 27% after one week and 8% after six months.8 This implies that dysphagia improves as time passes.8 Moreover, dysphagia in patients with stroke involving bilateral hemispheres is reported to be more severe and requires a longer period of time for recovery than stroke involving the unilateral hemisphere.8 In this case of unilateral stroke, dysphagia showed no improvement even after ten weeks. Therefore, although the patient had a definite history of stroke, other causes of dysphagia should be taken into consideration.
The retropharyngeal space is bordered anteriorly by pharyngeal muscle and fascia, and posteriorly by prevertebral fascia.9 This space includes no anatomically significant structures other than lymph nodes. These lymph nodes receive most lymphatic fluid from the head and neck, and degenerate after six years of age.10 Therefore there is a decreased incidencs of retropharyngeal abscess in adults. On the other hand, unlike adults, even healthy children are prone to a retropharyngeal abscess occurrence caused by upper respiratory infection, otitis media, pharyngitis and sinusitis. In adults, a retropharyngeal abscess usually occurs after dental treatment, trauma, swallowing of a foreign body, or are accompanied by underlying diseases leading to an immunocompromised state such as diabetes mellitus, malignant tumor and alcoholism.7 In this case, the patient had a history of diabetes mellitus, but the blood glucose level was well controlled, and there was no remarkable evidence of an immune disorder. Moreover, there were no predisposing factors like swallowing of a foreign body or surgical trauma such as a tracheostomy. Although surgery was performed for intracerebral hemorrhage, there were no signs of wound infection. In summary, there were no definite preceding causes for retropharyngeal abscess.
Possible symptoms caused by retropharyngeal abscess in adults include sore throat, dysphagia, cervical pain and rarely, airway obstruction. On diagnostic methods, a laryngoscopy may show normal results. Therefore lateral cervical X-ray imaging should be taken for the evaluation of retropharyngeal edema, and if a suspicious lesion is identified, a cervical CT or MRI examination must be performed in order to confirm the presence of an abscess and moreover, the predisposing factors.8 In this case, the patient had dysphagia and cervical pain. Retropharyngeal edema was identified on video fluoroscopic swallowing study performed for the purpose of evaluating dysphagia. Abnormal findings were present on laryngoscopy as well, and a cervical CT and MRI were carried out.
The causing organisms commonly reported are: group A β-hemolytic streptococci and staphylococcus aureus. Since gram negative bacilli and Mycobacterium tuberculosis could also be the causing organisms, a culture study along with additional examination for tuberculosis should be taken into consideration. Until the exact causing organism is verified, administration of broad-spectrum antibiotics is recommended.7 In this case, staphylococcus aureus was identified by culture study, and spondylitis was associated, which improved after the administration of intravenous Cefazolin 2 g every eight hours for eight weeks.
We presented a case of dysphagia caused by retropharyngeal abscess, rarely reported in adults to this day.
 XML Download
XML Download