

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Inadequate penile erection, also known as erectile dysfunction, is the most common sexual disorder in men. It is defined as the inability to achieve and maintain penile erection of adequate value to perform satisfactory sexual activity [1]. Erectile dysfunction can occur due to etiologies that are related to endocrinology, neurology, pharmacology, or vascular pathology, or can be psychogenic. Hemodynamic dysfunction is responsible for most of the cases due to venous incompetency or arterial insufficiency, with a relatively small number of patients suffering from a psychological etiology alone [23].
Although the exact prevalence of this disease in the male population is still not completely known, many studies have been conducted, with the Massachusetts Male Aging Study being the first large-scale community-based study of this pathology. This study reported the prevalence of erectile dysfunction to be 2.6% [4]. Another study reported the prevalence to be 52% among non-institutionalized males aged between 40 years and 70 years [5].
In patients having erectile dysfunction, it is important to differentiate a neurological or psychological cause from an organic cause. In addition to a comprehensive clinical history, physical examination, and appropriate laboratory investigations, color Doppler ultrasonography of the penis has become valuable in the evaluation of erectile dysfunction. It is a relatively inexpensive and minimally invasive tool that allows a good view of the penile anatomy [678], as well as the flow patterns in the vessels, in the diagnosis of erectile dysfunction [9]. This study was conducted with the aim of determining the frequency of organic and psychogenic causes of erectile dysfunction.
MATERIALS AND METHODS
This retrospective cross-sectional study was conducted at the Department of Radiology of Dow University of Health Sciences from July 2014 to June 2016. The condition of Institutional review board approval was waived as this was a retrospective study and all data were retrieved from electronic medical record. All patients who presented with erectile dysfunction and underwent a penile color Doppler examination with the injection of 20 µg of prostaglandin E1 during the study period were included in this study. The patients' previous medical records, detailed history, and other laboratory investigations were also reviewed at the time of the Doppler examination.
1. Penile Doppler procedure
A precise history was taken from every patient, and a peaceful surrounding with appropriate privacy was provided to relieve the patient's anxiety. Informed consent was obtained prior to the procedure. The examination was performed by a radiologist with more than 3 years of experience in ultrasonography. All the examinations were performed on GE Voluson S6 and GE Logiq P5 devices (GE Medical Systems, Milwaukee, WI, USA), with a high-frequency probe and the availability of color Doppler ultrasonography. Grayscale ultrasonography was performed in the transverse and the longitudinal sections to look for any abnormality. Following this baseline, the velocities of the right and the left cavernosal arteries were recorded before the injection. Spectral waveforms from the cavernosal arteries were measured at the base of the penis because it is the location with the highest velocities and the optimum angle correction.
On the basis of the baseline values, an intracavernosal injection of 20 µg of prostaglandin E1 was given close to the base of the penis. The peak systolic velocity and the end diastolic velocity were measured in each cavernosal artery at intervals of 5 minutes for a total of 30 minutes. Patients with a peak systolic velocity of less than 25 cm/s were considered to have arterial insufficiency. An end diastolic velocity of more than 5 cm/s was considered to indicate venous incompetence. Images were saved and printed on paper.
Erection grading of the penis at an interval of 10 minutes was done using the following erection hardness grading score [10]: 1, increase in the penis size but no hardness; 2, slightly hard erection; 3, sufficiently hard erection for penetration, but not fully hard; and 4, fully hard and rigid erection.
2. Statistical analysis
IBM SPSS ver. 20 (IBM Co., Armonk, NY, USA) was used for the statistical analysis. The mean and the standard deviation were calculated for quantitative variables, such as age, maximum velocity in the right cavernosal artery, and maximum velocity in the left cavernosal artery. The frequency and percentages were calculated for the causes of erectile dysfunction. An association of the cause of erectile dysfunction with the patient's age was observed. The chi-squared test was applied, and p-values <0.05 were considered significant.
RESULTS
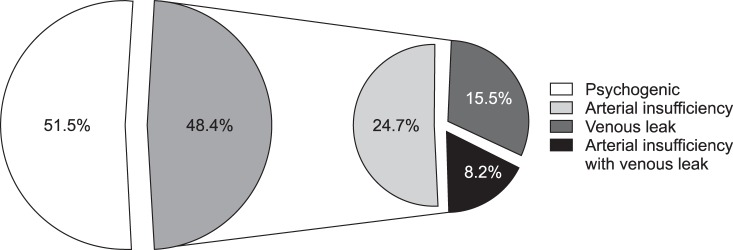
Out of 97 patients (mean age, 37.09±11.59 years; range, 19~69 years), 50 patients (51.5%) had normal penile Doppler ultrasonographic findings (maximum velocity in the right cavernosal artery: 46.22±18.41 cm/s at 16.1±7.34 minutes after the injection; maximum velocity in the left cavernosal artery: 48.07±20.87 cm/s at 17.59±7.02 minutes after the injection), 24 patients (24.7%) had arterial insufficiency (maximum velocity in the right cavernosal artery: 18.03±5.51 cm/s at 15.20±8.46 minutes after the injection; maximum velocity in the left cavernosal artery: 22.82±17.34 cm/s at 16.16±9.59 minutes after the injection), 15 patients (15.5%) had a venous leak (maximum velocity in the right cavernosal artery: 47.00±7.91 cm/s at 19.0±9.71 minutes after the injection; maximum velocity in the left cavernosal artery: 58.00±22.36 cm/s at 17.40±9.78 minutes after the injection), while 8 patients (8.2%) patients had arterial insufficiency with a venous leak (maximum velocity in the right cavernosal artery: 20.00±11.75 cm/s at 11.50±5.87 minutes after the injection; maximum velocity in the left cavernosal artery: 16.25±8.28 cm/s at 15.00±7.48 minutes after the injection) (Table 1, Fig. 1).
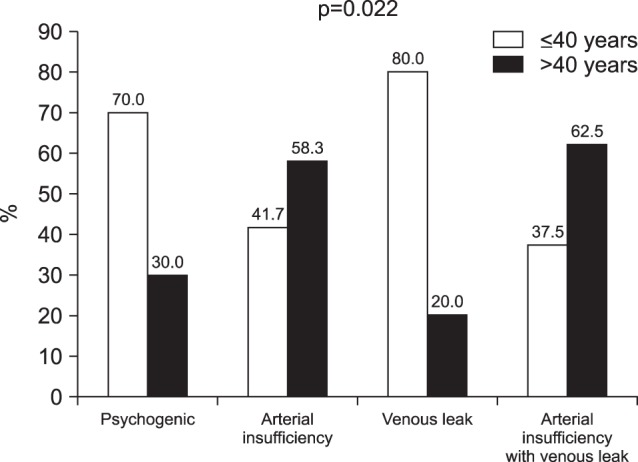
Age was significantly associated with the cause of erectile dysfunction (p=0.022) with a higher frequency of psychogenic causes in patients aged ≤40 years, while arterial insufficiency with or without a venous leak was higher among patients aged >40 years (Fig. 2).
DISCUSSION
In the evaluation of erectile dysfunction, color Doppler ultrasonography is a useful investigation for differentiating organic from psychological causes. With the advancement of the treatment options of male sexual dysfunction, this imaging modality will become important for the evaluation of the success rates of the treatment.
In this study, penile Doppler ultrasonography revealed a surprisingly high prevalence of psychogenic erectile dysfunction, as indicated by normal penile Doppler ultrasonography; this was found in the majority of the patients. This finding is similar to the findings of previous studies that reported a high rate of psychogenic erectile dysfunction using both similar and different techniques [1112].
In the present study, most of the patients suffering from psychogenic causes were younger than 40 years of age and had no known comorbidity. Upon taking a detailed history, we identified relationship problems after marriage and family pressures as the most important precipitating and maintaining factors for psychogenic erectile dysfunction. The demand for a premarital complete sexual check-up has now increased in our population, and this has led to a significant amount of stress in young men regarding failure to perform intercourse after marriage. In the existing literature, performance anxiety, that is, fear of failure during intercourse, has also been reported as a potential factor related to psychogenic erectile dysfunction. Further, multiple developmental, cognitive, affective, and interpersonal factors can predispose men to sexual dysfunction [2].
Among all organic causes, arterial insufficiency was found to be the most common in our study population. Organic causes of erectile dysfunction were more common in patients aged >40 years. The existing literature also states that the various risk factors of erectile dysfunction are associated with penile arterial insufficiency, including hypertension, hyperlipidemia, cigarette smoking, and diabetes mellitus [13141516]. Such disorders are highly prevalent in our community [171819]. Moreover, a relatively large number of cases of arterial insufficiency have been reported by other researchers [2021]. Another local study has also reported a relatively large number of cases of arterial erectile dysfunction, as compared to venous insufficiency [11].
Further, endothelial dysfunction is the common denominator of many vascular risk factors that can lead to arteriogenic erectile dysfunction [2223]. A previous study reported that erectile dysfunction improved when the concentrations of the elevated total and low-density lipoprotein cholesterol, were lowered either by dietary measures or by statin administration [2].
The findings of our study should be noted in the light of the following limitations. First, a psychogenic cause was determined based on the combination of the patient's history and normal ultrasound findings. We recommend identifying the cause-and-effect relationship of the psychogenic causes related to anxiety, depression, and other social factors, and research utilizing standardized questionnaires should be carried out for this purpose. The second limitation of this study is that the arterial velocities are the maximum near the base of the penis and decrease as they advance; operator dependency may have led to variability in recording the velocities. To minimize this variability, we need to record the velocities near the base of the penis where they are highest. Third, organic causes of erectile dysfunction were identified on the basis of color Doppler findings, and their relationship with risk factors such as hypertension, diabetes, and metabolic syndrome could not be clarified. Various studies have reported diabetes mellitus, hypertension, hyperlipidemia, metabolic syndrome, depression, and lower urinary tract symptoms to be causes of erectile dysfunction [213141516242526]. In this study, we were not able to determine the developmental cause of erectile dysfunction in the study population.
However, despite the abovementioned limitations, this study is a significant effort in reporting the outcome of penile Doppler ultrasonography from our developing country. Further prospective studies are recommended for the evaluation of causes leading to erectile dysfunction in our population. The higher frequency of psychogenic erectile dysfunction in this study suggests the need of psychosexual therapy in our population, particularly in people with significant psychological problems. Moreover, studies should be conducted to monitor the efficacy of psychosexual therapy in these patients. A recent systematic review also recommended that while treating erectile dysfunction, clinicians should ascertain the cognitive schemas, personality, sexual abuse history, and sexual expectations of the patients.
CONCLUSIONS
The higher frequency of psychogenic erectile dysfunction in a relatively younger age group suggests the need of psychosexual therapy in our population, particularly in patients with significant psychological problems. In the older age group, the predominant cause of erectile dysfunction was vascular problems. Early detection of psychogenic and vascular causes can lead to effective treatment and will ultimately eventually decrease the rate of infertility and depression among the population.

 XML Download
XML Download