

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Erectile dysfunction (ED) is a prevalent disorder affecting more than 150 million men worldwide [1]. The etiology of ED is multifactorial and its prevalence increases with age, particularly after the age of 60 years [23]. Risk factors and comorbidities associated with ED include cardiovascular disease, hypertension, diabetes mellitus (DM), tobacco use, hyperlipidemia, hypogonadism, lower urinary tract symptoms, metabolic syndrome (MetS), and depression [24].
The importance of addressing modifiable risk for men with ED has become increasingly evident, as we now know some interventions will improve multiple aspects of a patient's health [56]. A recent review by Gupta et al [7] found that lifestyle modifications targeting cardiovascular risk also had a positive impact on erectile function. The purpose of this review is to outline the most current literature assessing modifiable risk factors associated with ED, as well as to highlight interventions that may improve erectile function.
BACKGROUND ON ERECTILE DYSFUNCTION
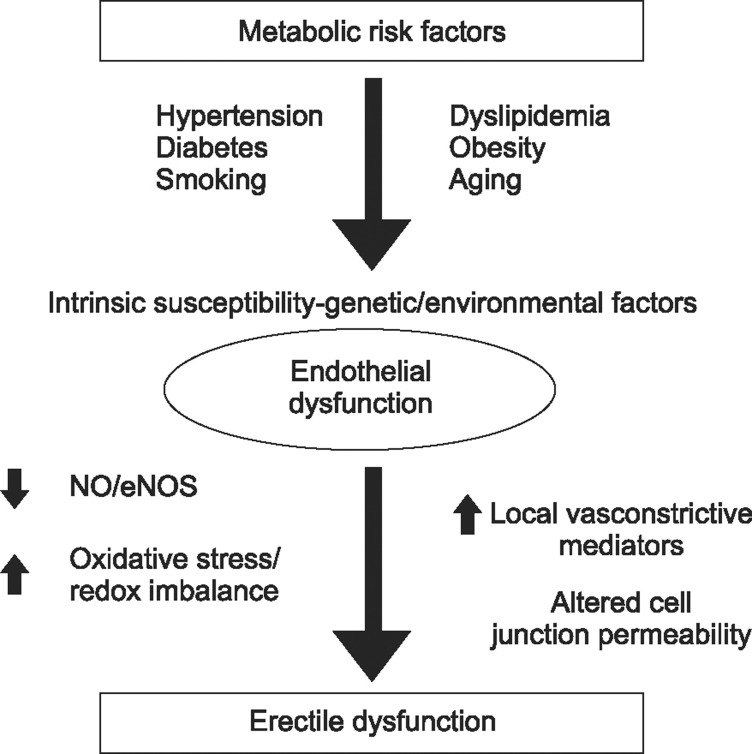
Erectile function is regulated by multiple body systems, including neuronal, hormonal, mechanical, and psychological. Nitric oxide (NO) is released by both endothelium and neurons, and stimulates guanylate cyclase to form cyclic guanosine monophosphate (cGMP). cGMP then relaxes vascular smooth muscle cells by activating protein kinases that impact multiple downstream effectors. While the exact mechanisms for the interaction of NO, cGMP, and corporal smooth muscle relaxation have not been fully elucidated, it is recognized that a healthy vascular endothelium can maintain good erectile function through regulation of vascular smooth muscle constriction and relaxation. However, when the endothelium is damaged by exposure to chronic disease and toxins, the vasculature can exhibit decreased production, impaired release, and increased destruction of bioavailable NO, thus leading to a disruption of the homeostasis typically demonstrated by healthy erectile tissue [89].
There are currently four common types of therapy utilized in the treatment of organic ED: oral drug therapy, vacuum tumescence devices, intracavernous vasoactive drug injections, and penile prosthesis implantation. Other therapies include psychosexual counseling, sex therapy, lifestyle changes, and gene therapy [10]. With a focus on risk factors and comorbidities that can be managed either medically or with lifestyle changes, the remainder of this review will focus on how the modification of specific risk factors can affect erectile function.
METABOLIC SYNDROME
MetS is a cluster of multiple medical issues—many of which will receive attention individually in this review— that negatively impacts erectile function. The Adult Treatment Panel III criteria, currently the most commonly used definition, state that MetS consists of at least three of the following five components: 1) central obesity, 2) hypertension, 3) increased fasting glucose levels, 4) elevated triglycerides, and 5) reduced high density lipoprotein cholesterol levels (Fig. 1). The epidemiologic link between MetS and ED is well established [11]. Given that the prevalence of MetS is approximately 35% in the United States, the relationship between MetS and ED is quite relevant. MetS affects erectile function both through inflammation and hormonal inadequacy [12]. Addressing the MetS requires a multifaceted approach with therapies including lifestyle modifications, testosterone replacement, clomiphene citrate, bariatric surgery, and pharmacotherapy directed at its individual components [13].
HYPERTENSION
Hypertension is a well-established risk factor for ED, with 30% to 50% of hypertensive men being affected [14]. The RhoA-ROCK pathway, which is involved in systemic hypertension, has been well established as an ED contributor [15]. There are downstream effects with subsequent decreased relaxation of the erectile tissues and collagen remodeling and fibrosis within the corpora cavernosa [16]. There are multiple other pathways linking hypertension and ED, including endothelial dysfunction, arteriosclerosis, and side effects from the medical management of hypertension.
While there is variability within each class of antihypertensive medications, it is well accepted that aldosterone receptor antagonists, beta-blockers, and thiazide diuretics have a negative impact on erectile function. Non-selective beta-blockers cause ED more frequently than selective agents such as metoprolol, which targets the beta-1 receptor.
Beta-blocking agents are a well-described cause of ED. Cordero et al [17] performed a cross-sectional study of 1,242 men treated with beta-blockers for ≥6 months. Surprisingly, they found that the men with adequate blood pressure control had a lower rate of ED, likely through improvement in endothelial function.
DIABETES MELLITUS
Diabetic men have a well-known increased risk of developing ED, with prevalence rates ranging from 35% to 90% [181920212223242526]. Additionally, diabetic men tend to develop ED 10 to 15 years earlier than the average ED patient [27]. They appear to present with more severe ED and suffer a greater diminishment in health-related quality of life components than the general population [28]. ED secondary to DM is more resistant to medical management with phosphodiesterase 5 inhibitors [29]. A systematic review by Binmoammar et al [30] of five cross-sectional studies found that poor glycemic control in patients with type II DM contributes significantly to the development and severity of ED. The reactive oxygen species generated as a result of hyperglycemia impacts multiple aspects of erectile physiology. The chronic complications of macrovascular changes, microvascular changes, neuropathy, and endothelial dysfunction increase the odds that a diabetic man will develop ED. Further, many men with type II DM ultimately experience the negative impact of MetS on erectile function [31].
The Diabetes Control and Complications Trial randomized 761 men with type I DM to intensive vs. conventional glycemic control at multiple institutions from 1983 to 1989. Patients were treated until 2003. At 10-year follow-up from trial termination, the men in the intensive glycemic control arm had a lower rate of ED (12.8% vs. 30.8%) [32].
Unfortunately, no data suggests that ED can be improved with strict glycemic control. The data on glycemic control before inflatable penile prosthesis implantation are conflicting. Interestingly, a prospective study by Wilson et al [33] failed to show an increased rate of inflatable penile prosthesis infection in men with a Hemoglobin A1c greater than 11.5%. Previously, Bishop et al [34] had shown a 31% infection rate if the A1c was greater than 11.5%, compared to a 5% infection rate if the A1c was less than 11.5%. Further studies are needed to clarify this discrepancy.
TOBACCO
Smoking causes oxidative stress and is a generally accepted risk factor for the development of ED [35]. A recent rat model documented several of the mechanisms that may be involved in ED and smoking. Rats exposed to 24 weeks of cigarette smoke had decreased penile neuronal NOS expression, decreased endothelial integrity, and diminished smooth muscle content compared to controls [36]. Smoking has also been shown to impair endothelial NOS-mediated vascular dilation in young men [3738]. In addition to the vascular damage associated with tobacco smoking, some data suggests that it may lower testosterone levels [39].
A review by Dorey [40] that examined 18 studies showed that smokers were 1.5 times more likely to suffer from ED compared to nonsmokers. This increased risk has been confirmed by multiple cross-sectional studies, with the increased risk varying from 1.5 to 3.1 fold when compared to nonsmokers [41424344]. It appears that the negative impact of smoking on erectile function is dose-dependent and cumulative. Studies have demonstrated that the increased risk of ED associated with smoking only becomes statistically significant after 20 pack-years or more [4546].
The data regarding smoking cessation and change in erectile function are conflicting. It is well established that smokers have a higher risk of ED at all points compared to those who have never smoked [47]. A study by Guay et al [48] performed nocturnal penile tumescence studies on men before and after 24 hours of smoking cessation. Improvement in erections was noted within 24 hours. Interestingly, a group of men who used nicotine patches showed improvement at 1 month. Pourmand et al [49] followed a group of patients presenting for nicotine replacement therapy to assist with smoking cessation. Data was collected on men with ED but no evidence of DM, hypertension, hyperlipidemia, or psychiatric disease. At one year, the International Index of Erectile Function (IIEF) scores were improved in 25% of men who managed to stop smoking while none of those who continued to smoke experienced improvement. It should also be noted that none of those who started with severe ED experienced improvement. In short, smoking increases the risk of ED and those who have mild to moderate ED may experience some improvement with smoking cessation.
HYPERLIPIDEMIA
Epidemiologic data has confirmed that hyperlipidemia is a strong independent risk factor for the development of ED via endothelial damage and inflammation [50]. The 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors (statins) are first-line medical therapy for hyperlipidemia and are protective of the vascular endothelium. In fact, statins have been shown to improve endothelial function prior to altering lipid levels [51]. There has been some conflicting data from individual studies; however, multiple meta-analyses have supported the conclusion that statins improve erectile function. A recent meta-analysis by Kostis and Dobrzynski [52] showed a 3.4-point increase in IIEF scores compared to controls. A separate meta-analysis by Cai et al [53] examined seven studies using two different statins and found a 3.27-point increase in IIEF scores.
OBESITY/DIETARY/PHYSICAL ACTIVITY
Physical activity counseling has been utilized in both the prevention of ED and the improvement of existent ED. The Massachusetts Male Aging Study (MMAS) followed 593 men, ages 40 to 70 years, with no prior history of ED, prostate cancer, heart disease, or diabetes for eight years. Physically active men showed a lower risk of developing ED [54]. This data has been supported by a recent meta-analysis of 11 studies showing that increased physical activity is protective against developing ED on multivariate analysis [55].
It can be difficult to identify the sole contribution of obesity to the development of ED, as it is often coexistent with DM and hypertension. Nevertheless, data does suggest that it has an independent contribution to ED. In the MMAS, obesity was an independent predictor of ED [54]. Multiple cross-sectional studies have shown that overweight (body mass index [BMI] 25~30 kg/m2) and obese (BMI >30 kg/m2) men have an incremental increase in the risk of ED with the relative risk ranging from 1.5 to 3.0 fold [56]. A prospective study by Esposito et al [57] randomized 55 men with ED to healthy behaviors (caloric reduction and consistent exercise) vs. control. At a 2-year follow-up, the treatment arm averaged 15 kg of weight loss with 31% regaining normal erectile function compared to 2% in the control arm.
A study by Kalka et al [58] demonstrated that patients with ischemic heart disease demonstrated limited knowledge about the association between modifiable risk factors and ED, particularly when questioned about sedentary lifestyle. If this finding holds true in other populations, patient education on lifestyle changes that promote weight loss and physical activity has the potential to reach a substantial number of patients.
HYPOGONADISM
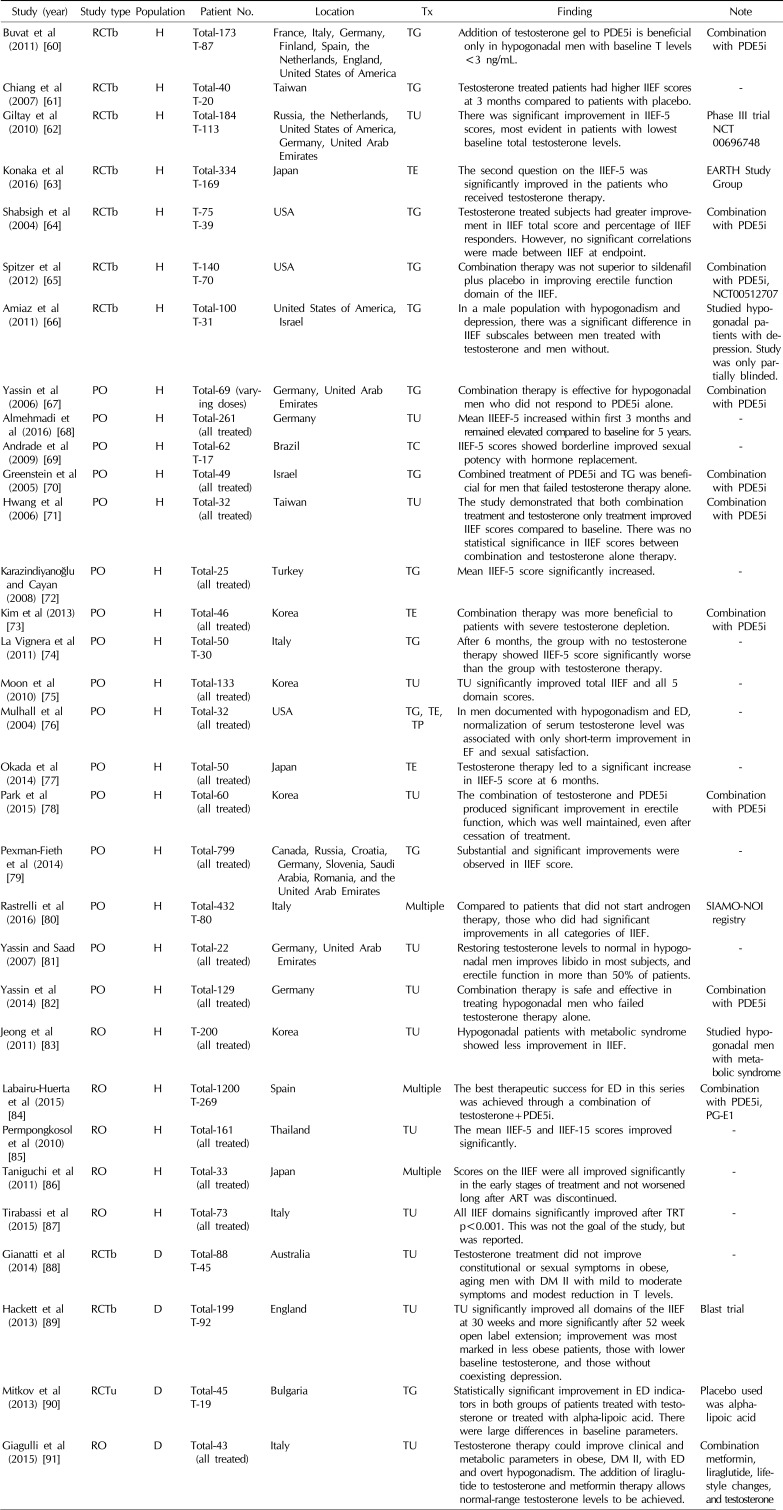
Testosterone is essential for adequate erectile function. The basic science literature has confirmed the necessity of androgens to generate adequate intracavernosal pressures and smooth muscle function to obtain an erection [59]. The literature showing the impact of testosterone replacement therapy (TRT) on erectile function is quite heterogenous (Table 1) [6061626364656667686970717273747576777879808182838485868788899091]. A subset analysis of the Olmstead County Cohort published by Gades et al [92] showed that testosterone has a statistically significant positive correlation with erectile function, even when adjusted for age. Multiple non-controlled observational studies have revealed that hypogonadal men treated with TRT have improved IIEF scores [687577]. Likewise, a randomized double-blind placebo-controlled trial of hypogonadal men given injectable TRT vs. placebo showed an improvement in erectile function in men on TRT [82]. A similar randomized double-blind placebo-controlled trial that observed hypogonadal men with type II DM showed no improvement in IIEF compared to baseline at 40 weeks of treatment [88]. Other observational studies have suggested that men with late-onset hypogonadism may not experience an improvement in erectile function after treatment with TRT [93]. It may be that the improvement in erectile function after TRT is transient. In a study by Mulhall et al [76], 32 men with ED and hypogonadism were treated with TRT and obtained physiologic levels of testosterone. There was a statistically significant improvement in erectile function, as measured by IIEF, at one month of follow-up, which was lost by 3 months. A recent meta-analysis by Corona et al [94] found a positive effect of TRT on hypogonadal men; however, this benefit was only seen in industry-sponsored studies. The recently published multicenter Testosterone Trial study provide solid evidence that TRT has a positive impact on overall sexual function in men 65 years of age or older. The Testosterone Trial, a multicenter randomized double-blind placebo-controlled study, consisted of three separate studies: The Sexual Function Trial, the Physical Function Trial, and the Vitality Trial. The sexual function trial showed that sexual activity and sexual desire were increased. Men in the TRT group reported significantly increased IIEF scores with a mean improvement of 2.64 points. This provides sound evidence that treating hypogonadism can improve erectile function [95].
DEPRESSION
There is a strong association between depression and ED, and it is not always clear which is the precedent condition. Furthermore, many of the treatments for major depressive disorders can cause ED. Cross-sectional data from the MMAS found that depressed men are twice as likely to have ED as the general population [96]. ED is a common side effect of selective serotonin reuptake inhibitors (SSRIs), with the incidence ranging from 20.8% to 80.3% depending on the medication utilized [97]. Recent data raises the concern that after SSRIs ED and genital anesthesia may persist upon discontinuation [98]. Bupropion, nefazodone, and mirtazapine are associated with a less than 10% incidence of ED, which is lower than that documented with standard SSRIs [99].
CONCLUSIONS
A great deal remains unknown about how lifestyle interventions affect erectile function. The risk factors mentioned in this review have been targeted as modulators of erectile function with varying degrees of success. Urologists need to counsel their patients on these risk factors, not only because of ED prevention, but also to impact on overall morbidity and mortality. Further studies are needed to clarify how much influence the modification of these risk factors can have on the amelioration and prevention of ED.
 XML Download
XML Download