

 PDF
PDF ePub
ePub Citation
Citation Print
Print


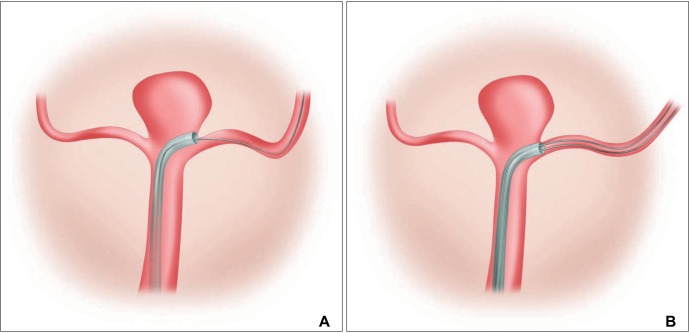
For the endovascular coiling treatment of wide-neck aneurysms, the use of a self-expanding stent has become part of the standard treatment [12]. There are several commercialized stents available and each stent has its own advantages and disadvantages [345]. One of the disadvantages of using an open-cell-design stent (Neuroform Easy; Stryker, Fremont, CA) though is the requirement for a large-bore microcatheter for delivery [67]. Even with the improved performance of the delivery microcatheter (Excelsior XT 27; Stryker, Fremont, CA), however, advancement difficulties are frequent due to a block at the transition between the distal margin of the aneurysm neck and the target branch vessel (Fig. 1A). This shortcoming has noted more often with wide-necked bifurcation aneurysms, such as those arising at the basilar top or at the middle cerebral artery (MCA) bifurcation aneurysms than with non-bifurcating ones, such as internal carotid artery (ICA) paraclinoid aneurysms (Fig. 1).
Because of this limitation, we previously had to switch to other types of stent that required a smaller profile microcatheter for delivery. We were able to overcome the delivery problem simply by introducing another microguidewire through the blocked microcatheter, which effectively minimized the diameter gap between the large-bore microcatheter and the microguidewire and decreased the acuteness of the arterial angle between the main parent artery and target branch vessel.
The purposes of this study is to summarize our experience of delivering the open-cell design stent for wide-necked bifurcation aneurysm coiling and to share our technical tip, which we refer to as the 'parallel-wire technique'.
MATERIALS AND METHODS
Patients
Between December 2014 and April 2015, we treated 15 cases of intracranial major bifurcation aneurysm: 8 basilar top, 3 MCA bifurcation, and 4 bi-hemispheric type anterior communicating artery (ACoA) origin aneurysms. This patient group comprised five men and 10 women with a mean age of 64.07 years (range, 46-77 years). Our local institutional review board approved our current retrospective study.
Procedure
After placement of a 6-Fr or 7-Fr guiding catheter, the stent was deployed before introducing a microcatheter for coiling into the aneurysm sac or after partial deployment of the frame coil (microcatheter jailing technique). For stent delivery, we used a 300-cm 0.014-inch microguidewire (Transend extra support; Stryker, Fremont, CA), which was placed into the target branch using an exchange technique. A 0.027-in microcatheter (Excelsior XT-27), which was designed for the stent, was advanced over the exchange microguidewire. To facilitate secure advancement of the largebore microcatheter, we tried to insert the distal end of the microguidewire deep into the peripheral cortical branch as far as possible. Once the Excelsior XT-27 microcatheter was placed successfully at the target stenting segment of the parent artery, a stent was deployed.
If we experienced any difficulty in advancing the microcatheter over the exchange microguidewire, we inserted a regular microguidewire (Traxcess 14, Microvention Terumo, Tustin, CA), which was used initially for the delivery of the regular microcatheter, into the Excelsior XT-27 microcatheter lumen along the already inserted exchange microguidewire in a parallel fashion ('parallel-wire technique', Fig. 1B). Then, the microcatheter navigated further into the branch over the two microguidewires. A stent was placed thereafter for subsequent coil embolization.
Analysis
We analyzed the initial technical success rate of delivering the Excelsior XT-27 microcatheter into the target vessel when the guidewire was used in a conventional way. We regarded a delivery procedure as failed, if the large-bore microcatheter could not be positioned properly for a stent placement. We analyzed the cause of initial delivery failure. On final control angiography after stent placement, we checked for the occurrence of any adverse procedure-related problem, such as vascular injury or vasospasm.
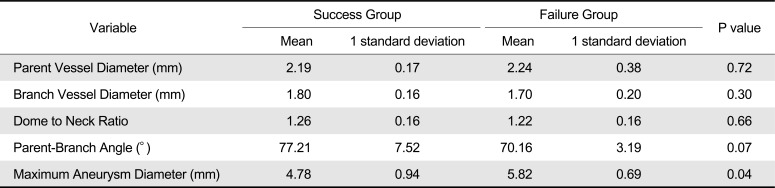
To detect any morphological differences in the parent artery, branching vessel, and the aneurysm itself between the success and failure group, we compared several morphological parameters. Using 3D angiographic images, we measured the dome-to-neck ratio, parent vessel diameter, target branch vessel diameter, parent to branch vessel angle, and maximum aneurysm diameter. Some of the parameters have been described previously [89]. We measured the maximum parent artery diameter at about 5 mm proximal to the aneurysm neck as the parent vessel diameter. The branch vessel diameter was measured as the maximum diameter of the target branch at about 5 mm distal to the aneurysm neck. The parent to branch vessel angle was measured on the same plane of the two vessels. The maximum aneurysm diameter was measured as the largest distance between any two points on the aneurysm dome.
The difference in morphological parameters between the success group and the failure group was analyzed. The statistical difference was evaluated with Wilcoxon signed-rank test using SPSS software version 21.0 (SPSS, Chicago, IL). The mechanism underlying microcatheter positioning failure and the success rate of the 'parallel-wire technique' were analyzed.
RESULTS
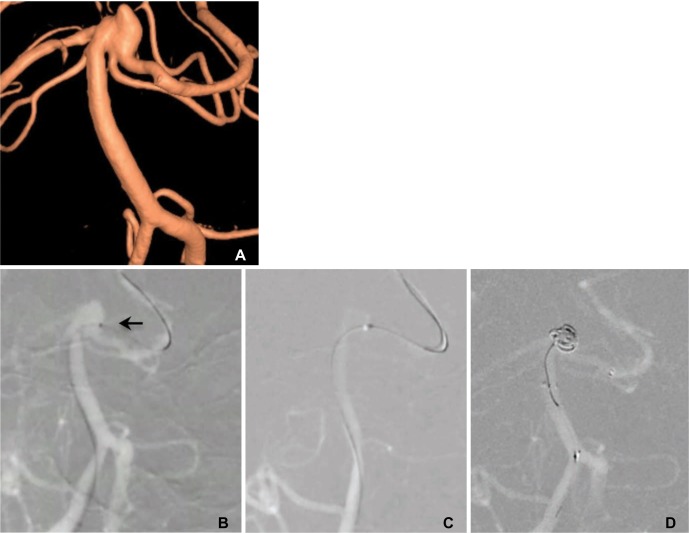
Navigation of the stent-delivery system into the target lesions was successfully performed using a standard technique in 10 of the 15 cases (66.7%). We had trouble with delivery wire advancement in five patients (33.3%, three basilar tip, one MCA bifurcation, and one ACoA lesion). The mechanism of advancement difficulty consisted of a block of the microcatheter tip due to a shoulder gap between the microcatheter outer diameter and the relatively smaller microguidewire thickness (Fig. 1A). In those five cases, we were able to advance the microcatheter successfully using the parallel-wire technique without any difficulty. The block disappeared as soon as a short segment of the second microguidewire tip advanced into the branching vessel (Fig. 2). Once the delivery catheter placed in the target vessel, the stent could position in the target sitesuccessfully in all five cases. There was no procedurerelated vascular injury or vasospasm on final control angiography.
The difference in the morphological parameters between the success group and the failure group is summarized in Table 1. We could not find any statistically significant difference except for the maximum aneurysm diameter (4.8 mm vs. 5.8 mm, p = 0.04).
DISCUSSION
We have found that difficulty in positioning the stent-delivery microcatheter is not an infrequent occurrence during the stent-assisted coiling of wide-necked aneurysms, especially in bifurcation lesions, such as basilar bifurcation or MCA bifurcation aneurysms. Personal communication with other experienced users of stent in coiling procedures revealed this to be a commonly experienced problem, and to be one of the reasons for not choosing this particular stent when technical difficulties with stent delivery were anticipated. We believe that our simple modification of our conventional stent delivery technique has solved the problem in delivering a large-bore microcatheter deep into the distal intracranial vessels.
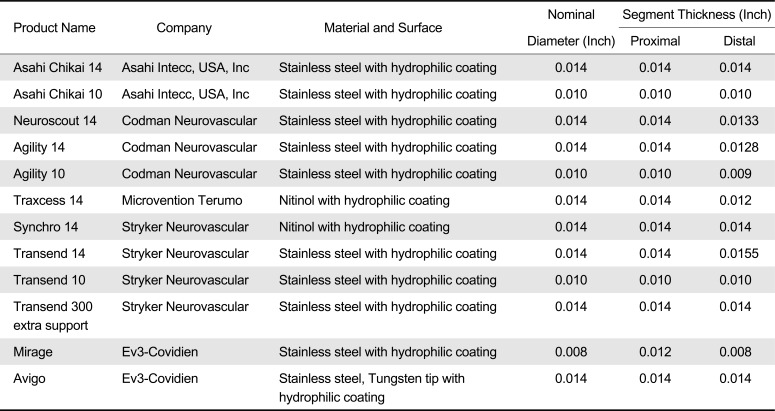
As for the detailed technique, the combination of microguidewires is potentially problematic. Since the inner diameter of the microcatheter is 0.027 inches, in theory the combined use of two 0.014-inch microcatheters would not be possible. However, the combined use of two 0.014-inch microguidewires was possible, since the nominal 0.014-inch size of the wire is compatible with a microcatheter that has an inner diameter larger than 0.014 inch. The actual diameter of a microguidewire can differ according to the segment and tends to be more slender distally. This was the reason why we could use the 0.014-inch Transend and the 0.014-inch Traxcess microguidewires together as described in the method section and in Table 2. We found that the distal usable part of the Traxcess was 0.012 inches and the real outer diameter of the Transend was less than 0.014 inches. However, we further found that the use of two Traxcess microguidewires was not possible, probably because of the thicker proximal segment design of the wire. We should take care in choosing the combination of microguidewires for their compatibility. Once the delivery microcatheter successfully placed in the target site, delivery of the stent is not a difficult task.
Although we did not include data on our present retrospective analysis, our technique could also be effective for side-wall aneurysms, especially those with a wide neck, such as cavernous ICA or paraclinoid ICA aneurysms. A good example could be a situation when a delivery microcatheter insertion is required for flow diversion of a large side-wall aneurysm. Since the inner diameter of the Marksman microcatheter (Covidien, Irvine, CA) is 0.027 inches, the same combination of microguidewire could be used.
In our present cases, ten of fifteen cases showed successful large-bore microcatheter delivery without the 'parallel-wire technique'. Although the small number of patients enrolled in our current retrospective analysis, we failed to demonstrate any geometric or morphological difference between the initial device delivery success and failure groups, except for the maximum aneurysm diameter (Table 1). One of the possible explanations for this finding is a change of geometry after successful insertion of the Transend microguidewire into the branching vessel. After straightening the target vessel, it became much easier to pass the large-bore microcatheter in some cases. Our current method consists of first attempting to pass the microcatheter over the single exchange microguidewire, and then, if there is any resistance at the tip, shifting to the parallel-wire technique and avoiding any second attempt over the single microguidewire.
CONCLUSION
Delivering a large-bore microcatheter for the stent-assisted coiling of a wide-necked, bifurcation aneurysm is a challenging step due to frequent blocking of the microcatheter tip at the ostium of the aneurysm. By parallel insertion of another microguidewire through the microcatheter, this block can be easily overcome and the microcatheter can thus be delivered to the target vessel.

 XML Download
XML Download